

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
BD affects ~ 1% of the population and shows strong heritability. Cytogenetic studies in psychiatry are important in view of the potential multiple etiologies of psychiatric syndromes and due to the high incidence of chromosome abnormalities reported in diverse psychiatry. The folic acid sensitive FSs in normal and abnormal populations remain unknown. It has been previously determined that there is a possible relationship which connects schizophrenia and folate.1 An analysis of FSs in bipolar and unaffected individuals showed a higher frequency of FSs at 1q32 in the bipolar population compared to the frequency of FSs in the controls using low folate media.2 Recent genetic studies have confirmed that susceptibility loci exist for BD on multiple regions of the human genome, including 4p14, 4q35, 6q24, 10p13-12, 12q24, 13q32, 16p, 18p11.2, 18q22, 20p11.2-q11.2, 21q21, 22q11-13, Xq, and Xq26.3-8 This data suggests that some chromosomal regions may play an important role in the genetics of BD.
In order to identify new or similar hot spots which are worthy of further study and that may be associated with BD, we reported our chromosomal findings from a control group of 40 patients with BD.
PATIENTS AND METHODS
A total of 40 patients who were diagnosed with BD [according to the DSM-IV criteria (American Psychiatric Association 1994)9] were recruited for this cytogenetic study. The patient group consisted of 23 males and 17 females. Their ages ranged from 18 to 47 years with a mean age of 32.61 ± 7.93 years. The patients were selected from a hospital for psychiatric and neurological diseases located in Adana, Turkey between October 2000 and December 2002. The study was granted ethical approval by the local health committee. The control group consisted of 34 healthy volunteers, 23 males and 11 females with a mean age of 37.13 ± 10.08 years.
Each sample was examined the for expression of folate-sensitive FS by the Faculty of Medicine in our Laboratory of Genetics at the Department of Medical Biology and Genetics, Çukurova University. The folate-sensitive FSs are likely to all be CCG repeat expansions similar to the fragile X. This is due to the abnormal expansion of genes with trinucleotide repeat polymorphisms, which have been found in bipolar affective disorder.10 These sites have longer, more complex repeat elements. Only two rare FSs (FRAXA and FRAXE) are of such unequivocal clinical significance that they are actually associated with intellectual disability. 11 Because of this, we used a folic acid-free medium (RPMI-1640, Sigma R6767 without folic acid) supplemented with 4% fetal calf serum, phytohemagglutinin, streptomycin, and penicillin. Standard cytogenetic techniques were used for harvesting and for slide preparation. Three slides were prepared for each subject. The slides were first stained only with Giemsa before examination in order to avoid the missing of any gaps. For detailed analysis of the FS, some slides were prepared by trypsin G-banding and at least 50 metaphases were scored for each assay. All gaps and breaks were recorded and localized according to the ISCN (1985).12 The classification of FS was done according to the nomenclature established in human gene mapping HGM 11.13
A non-parametric Mann-Whitney test was used for the statistical comparison of the means of chromosomal breaks and aberrant cells between patients and controls. The χ2 test was used to determine the difference in frequency of FSs observed between the patient and the control group.
RESULTS
A total of 2,033 cells from 40 patients with BD were analyzed for chromosomal FSs under treatment with folic acid-free medium. A total of 1,245 aberrations were found in 783 (38.5%) cells. In the control group, 297 aberrations were found in 262 (13.1%) cells among 2,000 analyzed cells. There was a significant difference in the total number of FSs expressed between patients and controls by the χ2 test (p < 0.001). No age and sex effects on FS expression were evident in our patients.
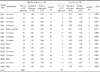
The analysis of the distribution of FSs on chromosomes showed that they were present in 1% of the cells analyzed and 15 of these different chromosomal FSs in the patient group included 10 c-fra [1p36(FRA1A), 1q21(FRA1F), 1q32(unknown), 3p 14(FRA3B), 5q31(FRA5C), 7q22(FRA7F), 7q32 (FRA 7H), 13q32(FRA13D), 14q24(FRA14C), and Xp22 (FRAXB)], 4 r-fra [11q23(FRA11B), 12q24(FRA 12D), 16q22(FRA16C) and Xq26(unknown)], and 1 previously unknown folate sensitive FS [3p25 (unknown)] (Table 1). Among these expressed FSs, there was a significantly higher frequency of 12 FSs at 1p36, 1q21, 1q32, 3p25, 7q22, 7q32, 11q23, 12q24, 13q23, 14q24, Xp22 and Xq26 in the patient group than in the controls, as determined by the χ2 test (p value between 0.001 to 0.036), excluding the 3p14, 5q31 and 16q22 regions (p value between 0.092 to 1.000) (Table 1).
DISCUSSION
Genetic factors are known to be important in the etiology of BD. The FS is a very interesting subject for the study of clinical disorders, because chromosomes have a tendency to break an FS, which can lead to the formation of deletions and translocations.14 The incidence of the folic acid-sensitive FSs in the BD remains unknown. The linkage findings in BD can be obtained from the collection of cytogenetic studies. Chromosomal regions of interest include 13q32, 1q32, 18p11.2, Xq26.3-q28, 4p16, 12q23-q24, 16p13, 21q22, Xq24-q26, Xq26.3,15,16 Our study represents the investigation of the possible involvement of chromosomal FSs in the etiology of BD.
In the present study, the frequency of FS was increased in lymphocyte cultures from patients with folate-sensitivity, which was significant when compared to the control group. It may be considered that the expression of c-fra could be an indicator of chromosomal instability. Of the 8 common and 3 rare FSs found in our study, 2 were listed in HGM11. 3p25 was neither in HGM11, nor reported previously. This site might be a novel folate-sensitive FS in BD. Of the FSs found in 33 cases (82.5%) out of 40 cases, c-fra at 1p36, 1q21, 1q32, 7q22, 7q32, 13q23, 14q24 and Xp22, and c-fra were expressed most frequently (Table 1). These sites may be hot spots for BD. Specifically, in our study, 7q22 expression was observed the most frequently with an incidence of 52%, followed by 7q32 (46%) (Table 1). A recent analysis has identified a locus on chromosome 7q for the language, and for repetitive or stereotyped behavior deficits.17 The results of two earlier genome scans has provided evidence for the involvement of 7q22 in schizophrenia.18,19 These independent results are consistent with the hypothesis related to susceptibility to BD.
We found three FSs on chromosome 1 at band 1p36, 1q21, and 1q32 that were significantly over-expressed in BD compared with the incidence of expression in controls (p = 0.002 - 0.016). Previous works have indicated a higher frequency of FSs at 1q32 in the bipolar patients when compared to controls.2,16 Similarly, evidence suggesting linkage to schizophrenia at the 1q21 - 22 and 1q32 - 41 loci has also been provided independently by three groups.20-22 It is interesting that the 1q21 site contains the locus of the dopamine receptor (DS) pseudogene I.23 The 1p36 site in our patients is a new class of FS, which have previously been called viral modification sites.24
The 11q23 site was also significantly over-expressed in our patients compared to the normal controls (p = 0.036). Linkage has been reported between bipolar disorder and chromosome 11.25-27 This rare FS was also observed in schizophrenic patients in another study.20 Published results of linkage studies of bipolar disorder have focused on chromosome 12q, where bipolar disorder was initially found to associate with Darier's disease,28 and the results of two earlier genome scans has provided evidence for the involvement of the 12q24 site for BD.8,16 The 12q24 and 13q32 expression have been observed most frequently in our patients (Table 1). Similarly, the 13q32 site has been also reported in bipolar patients.16,29
In our study, the X chromosome breaks and gaps were clearly clustered at Xp22 and Xq26. Linkage has been reported between bipolar disorder and loci on the X chromosome.30,31 Many of the genes along the X chromosome are expressed in the brain. The X chromosome includes the locus for other X-linked mental retardation (XLMR) syndromes. Mutations in any of these genes, which are essential for normal brain development and function, are potential causes of these XLMRs. Several linkage studies have provided evidence for a susceptibility locus related to bipolar disorder on chromosome Xq24 - 26, Xq24 - q27.1, Xq24 - q28 and Xq26.3 - 28.3,8,29,32 The higher expression of FSs along with the X chromosome mutations observed in our patients can lead to a local block of several genes in the regions around the FSs, leading to a variety of behavior disturbance in individuals.
The other chromosomal FSs at 1q21, 1q36, 3p25, 7q22, 7q32 and 14q24 were observed most frequently in bipolar patients in the present study. These FSs were not observed in other studies and may be new hot spots associated with BD.
In conclusion, it is still not clear whether an association between FS and BD can provide important knowledge in the search for the chromosomal location of major genes. Our findings suggest that these interesting regions may harbor important genes for BD and lead to a variety of behavior disturbance in individuals.
 XML Download
XML Download