

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Diabetic macular edema (DME) is the major cause of visual impairment in diabetic patients.1 Based on the observations of the Early Treatment Diabetic Retinopathy Study (ETDRS) Group, focal/grid laser photocoagulation has been the accepted standard care for DME. However, only 17% of eyes showed any improvement in visual acuity (VA), and less than 3% had visual improvements of three or more ETDRS lines after laser treatments.2-4 Moreover, a significant number of patients with DME, especially DME of the diffuse type, remain refractory to focal or grid laser treatments, and this has driven many investigators to seek alternative treatments for the management of DME.
Among alternative treatments currently under investigation, triamcinolone acetonide has been reported to be efficacious when administered either by the intravitreal route or a posterior sub-Tenon's route in cases of diffuse DME refractory to laser treatment.5-13 A previous report has shown, however, that intravitreal triamcinolone acetonide (IVTA) injection was more effective than posterior sub-Tenon injection of triamcinolone acetonide in the management of DME.14 Several recent reports demonstrated that PSTI was as effective as IVTA and could be accepted as a valid alternative to intravitreal injections.15,16 Grid treatment applied to areas of diffuse macular edema substantially reduces the risk of visual loss in eyes with DME.10,13 Thus, we hypothesized that grid laser macular photocoagulation might have an additive or synergistic therapeutic effect on posterior sub-Tenon triamcinolone injection.
In the current study, we prospectively investigated the efficacy and safety of IVTA treatment and posterior sub-Tenon triamcinolone injection combined with modified grid laser photocoagulation (PSTI + MP) in the management of diffuse DME.
MATERIALS AND METHODS
The study was a prospective, randomized clinical trial conducted at the Yonsei University Eye and Ear, Nose, and Throat Hospital (Korea) vitreoretinal service. The study followed the tenets of Declaration of Helsinki and was approved by the local Institutional Review Board. Informed consent was obtained from every patient after explanation of the nature and possible consequences of the study. Forty eyes of 33 patients with diffuse DME who visited our clinic from June 2005 to November 2005 were included in the study.
Patients
Patients were included in the study if they had DME arising from diabetic retinopathy, provided that the DME was of clinical significance by the ETDRS test, and also if they had generalized breakdown of the inner blood-retina barrier, as documented by diffuse fluorescein leakage on angiography and diffuse thickening of the retina, involving the foveal center and most of the macular area, on optical coherence tomography (OCT). The exclusion criteria were (1) a prior history of vitrectomy, (2) intraocular surgery other than vitrectomy, including cataract extraction, within the 6 months prior to potential enrolment, (3) laser treatments including panretinal photocoagulation, posterior capsulotomy, or focal/grid macular photocoagulation within the 6 months prior to potential enrolment, (4) presence of ischemic maculopathy documented on preoperative fluorescein angiography, (5) prior history of elevated intraocular pressure (IOP) secondary to steroid treatment, (6) history of glaucoma or ocular hypertension, or (7) presence of comorbid ocular conditions that might affect VA.
Ophthalmic examinations to evaluate macular edema were performed using 90+ diopter noncontact lens slit lamp biomicroscopy. Fluorescein angiography, color fundus photography, and Third Generation OCT (OCT3, instrument from Stratus Zeiss Humphrey, San Leandro, CA, USA) were performed by the same experienced masked ophthalmic technician. For each patient, the best corrected VA was determined with the ETDRS chart.17 Foveal thickness was measured by OCT using the Fast Macular Thickness scan. IOP was measured using a Goldman applanation tonometer. Cataract progression was determined according to the Lens Opacities Classification System III (LOCS III) grading system.18 Patients were monitored for potential injection-related and laser-related complications. Examinations were carried out at baseline and also at 1 month, 3 months, and 6 months after treatment, and the results were evaluated by the same masked retinal specialist (HL). The patients' treatment groups were masked during follow-up visits.
Surgical procedures
Forty eyes of 33 patients were randomly allocated into one of two treatment groups by a permuted block randomization. A total of 20 eyes received PSTI + MP treatment, and the second group of 20 eyes received IVTA treatment. After randomization, treatments were carried out by the same retinal specialist (HJK).
The IVTA group received intravitreal injection of 4 mg/0.1 mL triamcinolone acetonide (40 mg/ml; Tamceton®; Hanall Pharmaceutical, Seoul, Korea). The injections were performed using 0.5% (w/v) proparacaine drops (Alcaine; Alcon Laboratories, Fort Worth, TX, USA) for topical anesthesia under sterile conditions. The drug was injected through the inferotemporal pars plana using a 30 gauge needle. The appropriate intravitreal localization of the suspension and perfusion of the optic nerve head were confirmed by indirect ophthalmoscopy.
Each patient in the PSTI + MP group who received a posterior sub-Tenon triamcinolone injection after macular photocoagulation had been performed earlier on the same day. We performed macular grid photocoagulation on spots 100 µm in diameter, with width spacings of 1 - 2 burns, an exposure time of 0.1 - 0.2 sec, and a laser power of 100 - 150 mW. Grid laser photocoagulation was performed by placing medium white laser burns over the entire areas with thicknesses of ≥ 350 µm, as documented on OCT Fast Macular Thickness scans. Laser treatment over papillomacular bundles was avoided. Posterior sub-Tenon triamcinolone injection was performed after laser photocoagulation. Before injection, 0.5% (w/v) proparacaine drops were applied and 40 mg of triamcinolone acetonide (1 mL) was injected with a 25 gauge, 5/8-inch-long needle attached to a tuberculin syringe. The superotemporal conjunctival fornix was penetrated with the needle, and the drug was injected.19
Measurements of primary outcome
The measurements of primary outcome included best-corrected ETDRS VA scores and foveal thicknesses measured by OCT. Each ETDRS VA score was measured by a masked investigator by determining the number of letters which a patient was able to read from the ETDRS charts with correction for individual refractive errors. The main outcome measurements were performed at baseline and at 1 month, 3 months, and 6 months after treatments. Secondary endpoints were complication rates, as evaluated by IOP measurements, cataract progression, and injection-related ptosis (measured by the distance between the reflection from the corneal apex and the upper eyelid).
Sample size calculation
After considering the results of previous studies and our preliminary data with intravitreal and posterior sub-Tenon drug injections for DME, we concluded that a sample size of at least 18 eyes per treatment group offered a probability of 80% for detection of a 35% reduction in macular thickness at the 0.05 significance level (2-sided).5,6 We estimated 10% follow-up loss of patients during the study, and therefore our goal was to recruit 20 eyes for each group.
Statistical analyses
Baseline demographic and clinical parameters were compared between treatment groups using Student's t-tests for continuous variables and chi-square tests for categorical variables. The study endpoints were analyzed using repeated measures ANOVA, which was adjusted for correlations of subjects within a group and group/time interactions. Between-group comparisons at each time point were performed using Student's t-test. In addition, paired t-tests were utilized to compare differences between each follow-up time point and baseline values within each treatment group.
Statistical analyses utilized SPSS® 12.0.1 (SPSS Inc., Chicago, IL, USA) for Windows. The level of statistical significance was set at p < 0.05. For within-group comparisons, the significance level was adjusted to take the number of comparisons to baseline into account (α = 0.05/3 = 0.0167; Bonferroni's adjustment for multiple comparisons).
RESULTS
The baseline characteristics are listed in Table 1, there was no statistically significant difference between the 2 groups. All randomized eyes followed assigned treatments to the end of the study.
Early Treatment Diabetic Retinopathy Study score
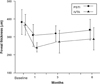
Repeated measures ANOVA showed a sig nificant effect on VA with either treatment (p = 0.03) and over time (p < 0.001). No significant treatment/time interaction was found (p = 0.53). Fig. 1 and Table 2 present, the mean changes in ETDRS scores at baseline and at 1 month, 3 months, and 6 months after treatment. Within each treatment group, pairwise comparisons revealed significant improvements in ETDRS scores after 1 month and 3 months (all p < 0.016, using the Bonferroni adjustment; significance level = 0.0167). The VA improvements were no longer statistically significant at 6 months in either group. Between-group comparisons revealed no significant differences in changes of ETDRS scores from baseline at any timepoint.
In patients who had visual improvement, 10 of 20 eyes (50%) in the PSTI + MP group and 11 of 20 eyes (55%) in the IVTA group showed an increase of more than one line in ETDRS scores at 6 months after treatment (p = 0.75).
Foveal thickness
Repeated measures ANOVA showed a significant effect of either treatment on mean foveal thickness (p = 0.01), over time (p < 0.001). No significant treatment/time interaction was found (p = 0.56). Fig. 2 and Table 3 present the changes of mean foveal thicknesses at baseline and at 1 month, 3 months, and 6 months after treatments. Pairwise comparisons revealed significant improvements in average foveal thicknesses at 1 month (p = 0.01) for the PSTI + MP group, and at both 1 month (p < 0.001) and 3 months (p = 0.016) for the IVTA group. Between-group comparisons revealed no significant differences in changes of foveal thicknesses from the baseline at any timepoint.
Complications
Fig. 3 and Table 4 present changes of mean IOP from baseline at 1 month, 3 months, and 6 months after treatments. Between-group comparisons revealed significant differences in mean IOP changes at 1 month and 3 months (p = 0.006, p = 0.026, respectively). Three of 20 (15%) eyes in the IVTA group developed IOP elevation which exceeded 21 mmHg; and this was controlled with topical anti-glaucomatous agents. The 3 eyes with elevated IOP belonged to three different patients. No eye that received a posterior sub-Tenon injection developed increased IOP exceeding 21 mmHg.
One of 20 (5%) eyes in the PSTI + MP group showed a complication of mild ptosis that gradually improved towards the end of the study. According to the LOCS III scoring system, the average increases in cataract grading, compared to baseline values, were 0.62 ± 0.81 (mean ± SD) in the PSTI + MP group and 1.54 ± 1.33 in the IVTA group; the latter was significantly higher than the former (p = 0.043, Student's t-test). Significant cataract progression that necessitated cataract surgery was noted in 1 of 13 (7.7%) phakic eyes in the IVTA group, but in none of the eyes treated with posterior sub-Tenon injections. The cataract complication that occurred after IVTA administration was treated with extracapsular phacoemulsification and posterior chamber intraocular lens implantation after the end of the study.
Serious vision-threatening complications, such as infectious endophthalmitis, vitreous hemorrhage, scleral perforation, and retinal detachment, were not encountered in any study eye.
DISCUSSION
In recent years, application of triamcinolone acetonide via either an intravitreal or a posterior sub-Tenon's route has yielded promising results in the treatment of diffuse DME refractory to laser treatment.5-9
IVTA has become an increasingly popular mode of DME treatment, and may be used after failure of initial laser treatment, or, indeed, instead of laser treatment as the primary therapeutic modality in some cases.20,21 The effects of corticosteroid delivered by IVTA treatment do not last longer than 6 months, and recurrence of macular edema often requires repeated IVTA applications.5,6 The problem with repeated intraocular injections of triamcinolone acetonide is that patients become predisposed to the cumulative risk of injection-related complications such as cataract progression, infectious endophthalmitis, intraocular hemorrhage, retinal detachment, and glaucoma.5-7,22-24
The advantages of periocular administration of triamcinolone include lower risks of endophthalmitis, cataract progression, and IOP elevation, and the delivery of triamcinolone via the sub-Tenon route may offer a safer alternative to intravitreal injection. However, a previous study compared treatment results in patients with diffuse DME after intravitreal injection and sub-Tenon's infusion of triamcinolone acetonide, and suggested that IVTA treatment might be more effective than PSTI. On the other hand, some other studies demonstrated that PSTI would be a valid alternative to the IVTA.14-16 Thus, we performed modified grid laser macular photocoagulation on the same day when PSTI was performed, to take advantage of additive effects of the laser and drug treatments previously reported.10,13 We identified retinal areas with diffuse thickening (prior to modified grid laser treatment) using the OCT Fast Macular Thickness scan, because several studies demonstrated that OCT detects foveal thickening in DME with a sensitivity better than that offered by clinical examinations.25-29 Grid laser photocoagulation was performed on the same day as PSTI treatment in the current study. A question of whether grid laser treatment applied a few weeks after steroid administration would result in even better results should be determined in further studies.
In our study, both treatment modalities showed significant treatment effects over a 3 month period. Although the difference was not statistically significant, there was a small vision imbalance at baseline, with the PSTI + MP group having better vision. As shown in Table 2, the changes of vision properties from baseline at 1 month and 3 months after treatments were, nonetheless, comparable between the 2 groups. Our current results seem to contradict a recent report by the Diabetic Retinopathy Clinical Research Network.30 These authors reported in a pilot study that peribulbar triamcinolone with or without focal photocoagulation was unlikely to be of substantial benefit in the treatment of mild DME in patients with VA scores of 20/40 or better. The apparent disparity may arise because of differences between the patient groups treated in the 2 studies. In the cited work, patients with mild DME and relatively good VA values were included. On the other hand, only 4 of 40 eyes (10%) had baseline VA values of 20/40 or better in our current study, and all our patients had DME of the diffuse type. Because a previous study showed that worse baseline VA values in DME patients were associated with better visual outcomes after IVTA treatment, and that patients with particularly poor VA scores may benefit most from the treatments which we employed.31
The duration of the treatment effect seemed to be longer in the IVTA group, since the mean ETDRS score began to decline after 3 months in the PSTI + MP group, but remained relatively stable to 6 months in the IVTA group, however, the difference was not statistically significant. By 6 months, the PSTI + MP group showed visual outcome similar to that of the modified grid laser, a standard care for diffuse DME, with 5 letters improvement, indicating that repeated PSTI might be necessary to maintain optimal treatment outcomes.32,33 The IVTA group also showed a longer mean duration of resolved macular edema, since a significant change in mean foveal thickness was apparent 3 months after treatment. This improvement gradually decreased, however, and was no longer significant by 6 months post-treatment. Because the functional and tomographical outcomes in both treatment groups started to decline by the end of the study, the effect of triamcinolone delivered by either route appears to be transient. Although the interval required between injections may average longer in IVTA patients under continuous ophthalmic care, repeated injections would still be necessary for patients treated with either modality. It is beyond the scope of the present study to determine whether IVTA combined with grid laser photocoagulation would result in a longer-lasting effect. Further studies on this issue are warranted.
When complications were considered, we observed a higher mean increase in IOP from baseline at 1 month and 3 months and a 15% rate of IOP elevation requiring anti-glaucomatous treatment in the IVTA group, whereas no eye of the PSTI + MP group showed a significant elevation of IOP. The IVTA group also showed significantly higher average increase in cataract grading. The frequency of significant cataract progression requiring surgery (7.7%) in this study was within the range (0 - 23%) of previously reported incidences.5-8,34-36 Considering the relatively short follow-up period of this study, it should be mentioned that a higher rate of cataract progression might be observed in the IVTA group upon longer-term follow-up of patients.
Some limitations of our study are inherent, and include possible confounding influence of cataract progression on VA scores in the IVTA group, our small sample size, limited duration of follow-up, and a lack of proper control group. We observed a significant increase in average cataract grading in the IVTA group, and the mean VA effect in the IVTA group might be underestimated because of lens opacification that was not considered to be of sufficient clinical significance to merit surgery at the time of observation. Since the modified grid laser treatment has been a standard care for diffuse DME and the grid laser photocoagulation combined with IVTA has also shown promising results,37 a control group treated with either conventional laser treatment or IVTA combined with MP would be necessary to verify the current findings. The current study is also limited by the lack of information regarding the systemic factors that might have influenced the progression of DME, such as the use of insulin therapy, oral hypoglycemic drugs and the status of glycemic control. Further studies with larger group sizes, proper control group and detailed information regarding systemic factors are necessary to evaluate the long-term therapeutic effects, possible side-effects, and appropriate drug dose, when PSTI + MP is used for the treatment of DME.
There were seven bilateral DME cases; three in the PSTI + MP group and four in the IVTA group. We repeated all statistical analyses, including only the right eyes of these patients to eliminate any possible influence of contralateral effects in either treatment. The results obtained were similar to those discussed above and therefore, were not considered any further.
In summary, our pilot study suggests that PSTI + MP treatment provides vision improvements in patients with diffuse DME, similar to those obtainable with IVTA treatment, and that the effects last for 3 months with fewer complications than seen in patients receiving IVTA treatment. Further studies using macular grid photocoagulation with repeated injections of 40 mg of triamcinolone into the posterior sub-Tenon's capsule at 3 months intervals are, therefore, indicated.






 XML Download
XML Download