

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Urachal anomalies are rare in adults. In particular, reports of urachal cysts containing stones are extremely rare. This complicated urachal anomaly requires a surgical excision to prevent symptomatic recurrence and malignant degeneration. 1 However, traditional open excisions are associated with significant morbidity and prolonged convalescence.2
We report a case of a stone-containing urachal cyst, and aim to discover whether laparoscopy is possible for the treatment of complicated urachal disease as a minimal invasive surgery.
CASE REPORT
A 58-year-old man presented with lower abdominal pain and urinary frequency for 1 month. Physical examination was unremarkable. Routine laboratory examinations of blood showed no abnormalities. Urine analysis revealed a high number of red blood cells and 1 - 3 white blood cells per high power field.
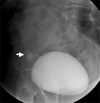
Plain x-ray films demonstrated radio-opaque densities in the pelvic area. Ultrasonography showed hyperechoic calcifications in a cystic lesion in front of the bladder. Cystography revealed radio-opaque stones of 1.8 × 1.3 cm and 0.6 × 0.3 cm in the pelvic cavity, which was separated from the bladder (Fig. 1). Abdominal computed tomography showed hyperdense stones in the urachal cyst (Fig. 2). We performed a cystoscopy and could not find the opening to the urachus. We diagnosed him with a urachal cyst with stones. He underwent laparoscopic excision of the urachus with a transperitoneal approach.
The patient was placed in a supine position. Pneumoperitoneum was established with a Veress needle. Three trocars were inserted into the peritoneal cavity, including a 10-mm trocar for a camera located three fingers above the umbilicus in the midline, a 10-mm trocar in the right pararectal area, and a 5-mm trocar in the left pararectal area at the level of the umbilicus.
The cephalic side of the urachus was dissected from the umbilicus with ultrasonic scissors. The caudal stump of the urachus and dome of the bladder were excised and repaired by running 3 - 0 polyglactin. The specimen was removed with a laparoscopic retrieval bag through the 10-mm trocar site.
The total operative time was 110 minutes. The blood loss was 50 mL. There were no operative complications. The patient ambulated and resumed oral intake on postoperative day 1. The urethral Foley catheter was removed on postoperative day 5. The patient was discharged 7 days postoperatively.
On pathologic examination, the urachal cyst was filled with brownish stones, and weight of the specimen was 69 gm. Examination revealed a benign cyst with nonspecific inflammation. The final diagnosis was an inflammed urachal cyst containing stones (Fig. 3).
DISCUSSION
The urachus is an embryonic connection between the allantois and the anterior part of the bladder dome. It lies between the medial umbilical ligaments. Common abnormalities of the urachus are a patent urachus, urachal cysts, or a urachal sinus.
Urachal cysts are the result of persistent epithelial lining of the lower third of the urachus. These are found in 1 in 5000 births, with a male to female ratio of 3 : 1.3 These anomalies are extremely rare in adults; most are detected in childhood as a result of infection. In addition to their relative rarity in adulthood, the difficulty in accurately identifying these entities is largely a result of their varied presentation. They may present as calcification of the cyst wall or as stone formation within the cyst.4,5 About 10% of the cases were associated with stones. Usually, the stones are less than 10 mm in size.
In the reported cases of the urachal cysts containing stones, the patients were 40 to 74 years old. Male patients were reported more frequently. The symptoms included lower abdominal pain, irritative voiding symptoms, and a palpable abdominal mass with or without umbilical discharge.4-7
Several radiographic tests and cystoscopic investigation are needed to confirm the urachal anomaly. However, it is difficult to find a obvious connection between the bladder and the urachus.
Resulting complications include secondary infection, peritoneal rupture, cancer, fistula, acute hemorrhage, urinary or intestinal obstruction, and Reiter syndrome.1,8
Traditional management of this lesion includes radical excision of all urachal remnants with or without a cuff of bladder tissue. It can be performed with an open or laparoscopic approach. Open surgical removal of the urachal cyst requires a transverse mid-hypogastric or vertical incision.2 Recently, laparoscopic surgery has become popular in the urologic field as an alternative minimal invasive approach.
Neufang et al. reported the first laparoscopic excision of a urachal remnant in 1992.9 Since then, Jorin et al. and Siegel et al. have reported laparoscopic excision of a urachal cyst, and several reports on the laparoscopic surgery have demonstrated an excellent outcome with minimal invasive surgery.10
Our rare case of a urachal cyst containing stones in an adult is unique for several reasons. The stones in the urachus were larger than those in previous reports. Also, the urachus was excised with the bladder cuff laparoscopically. Laparoscopic excision of the urachal cyst containing stones has not been extensively presented in the English-language literature to the best of our knowledge. It appears that laparoscopic excision is a safe and less invasive method (including smaller operative scars and early recovery) for the treatment of such complicated urachal anomalies.


 XML Download
XML Download