

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Epidemiological and experimental studies both in vivo and in vitro suggest that fecal bile acids (FBAs) may play a role in the etiology of colorectal cancer.1-4 It has previously been shown by Hill et al,1 in England and Reddy and Wynder5 in the United States that the mean concentration of total FBAs in patients with colon cancer were higher than those in control subjects, however, further studies failed to demonstrate similar results, raising some doubts over the proposed implication of bile acids.6,7
Large bowel carcinogenesis is a multistage process involving the formation and growth of the adenoma, development of increasingly severe epithelial dysplasia, and finally the progression to malignancy; this process is referred to as the adenoma-carcinoma sequence.8 In other words, colorectal adenomas are well-established precursor lesions for colorectal cancer. Then, the value of individual bile acids as a potential risk marker for colorectal cancer can be further evaluated by study of FBA profiles in patients carrying colorectal adenoma. For bile acid metabolism, many studies reported that patients with colorectal adenoma also had an increased proportion of DCA in their feces.5,9 However, these studies have been limited by small sample size. A meta-analysis may provide a more precise understanding of the true effect. Here, we performed a meta-analysis of all eligible studies in order to address the relationship between FBAs and colorectal cancer or adenoma.
MATERIALS AND METHODS
Data sources and searches
Electronic databases (Pubmed, Embase, Cochrane Controlled Trials Register, Science Citation Index, and Chinese Biomedical Database) were searched up to March 2007 for all observational studies that examined the relationship between bile acids and colorectal cancer or adenoma. For the search, we used both medical subject headings, textwords, and their abbreviations: "bile acid", "cholic acid", "chenodeoxycholic acid", "deoxycholic acid", "lithocholic acid" and "ursodeoxycholic acid" in combination with "colon cancer", "colonic cancer", "rectal cancer", "colorectal cancer", "adenoma", and "adenomatous polyps". Both literature searches were limited to "human" and "English language", except for Chinese in the Chinese Biomedical Database. We also performed a manual search of references cited by the original published studies and relevant review articles. Authors of some identified trials were asked whether they knew of additional studies including unpublished ones.
The contents of abstracts or full-text manuscripts identified through the literature search were reviewed independently by 2 investigators (Tong JL and Shen J) in duplicate to determine whether they met eligibility criteria for inclusion. When discrepancies between investigators occurred for inclusion or exclusion, a third investigator (Ran ZH) was involved to conduct additional evaluation of the study and discrepancies were resolved in conference.
Inclusion and exclusion criteria
For inclusion in the meta-analysis on the mean concentrations of bile acids and colorectal cancer, studies had to have an analytical design (case-control, cohort, or cross-sectional) and examine the relationship between bile acid concentrations and colorectal cancer or adenoma. Studies were included only if they were published as full-length articles or letters in peer-reviewed journals. All studies were required to have extractable data. Data expressed as medians were not included in the meta-analysis. For total or individual bile acids, data reporting concentrations of bile acids in fecal water were also not included. For duplicate publications, the smaller dataset was excluded. In all searches, we contacted the authors to obtain the required information when relevant information was not reported or there was doubt about duplicate publications.
Data extraction
All data were independently abstracted in duplicate by 2 investigators (Tong JL and Shen J) using a standardized data collection form. Discrepancies were resolved by discussing with a third investigator (Ran ZH). Study characteristics recorded were as follows: first author's name, year and source of publication, country of origin; inclusion, exclusion criteria, outcomes, number enrolled, mean age in each group, percentage of females, number of control case groups, mean levels of total bile acids, CDCA, DCA, LCA, and primary and secondary bile acids.
In the case of trials with more than 2 groups, and dichotomous outcomes, both the number of events and total number of patients would be halved; for continuous outcomes, only the total number of participants would be halved.
Statistical analysis
Some of the studies included in our meta-analysis differed in the unit used for reporting levels of total bile acids (µmol/g vs. mg/g). Therefore, we converted all units to mg/g using the conversion factor 1 µmol/g = 0.385 mg/g for total FBAs.
We calculated the WMD and 95% CI for all variables. The inverse variance method was used to weight the studies. A fixed-effects model approach was used but in case of heterogeneity, a random-effects model was used. We assessed heterogeneity with I2, which describes the percentage of total variation across studies because of heterogeneity rather than chance. Negative values of I2 are put equal to 0. I2 lies between 0% (no observed heterogeneity) and 100%. I2 values of 50% and more indicate a substantial level of heterogeneity. The heterogeneity between groups (cancer and adenoma) was also calculated using chi-squared test and significance was set at p < 0.10. For subanalysis, we calculated the WMD and 95% CI by geographical location (Europe, Asia, North America, and other continents) and lesions (cancer vs. adenoma). Publication bias was assessed with funnel plot. Begg and Egger tests were also performed. All analyses were performed with the statistical package Stata (ver. 9, Stata Corp., College Station, TX, USA) using the "metan" and "metabias" commands. For forest plots, the size of the box for each study represents the weight of the study in the meta-analysis. The lines around the point estimate represent the 95% CI for the individual studies. The diamonds represent summary estimates from the meta-analysis; the width of the diamond is the 95% CI.
RESULTS
Description of studies
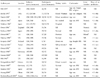
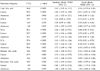
The bibliographical search resulted in 941 hits. Of these studies, only 19 investigated the relationship between FBAs and colorectal cancer or adenoma. In addition to this, 1 study was identified in the Chinese Biomedical Database. Finally, 20 studies including a total of 1,226 individuals fulfilled our inclusion criteria. The flowchart of reviews showed the detailed process of selection (Fig. 1). Of the articles included, 18 were case-control1-3,10-24 and 2 cohort designed.25,26 Among the 20 studies, 7 were conducted primarily in the United Kingdom, 4 in Japan, 2 in France, 2 in Germany, 1 in the United States, 1 in Finland, 1 in Northern Ireland, 1 in Greece, and 1 in China. Table 1 summarizes the characteristics of the 20 trials included in the review. Table 2 shows the Q-statistics and I2 statistics for the overall analyses and compared the results of random effects to fixed effects models.
Total bile acid
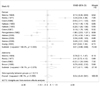
Nineteen studies reported extractable data about the relationship between total FBAs and cancer/adenoma of the large bowel. No association was seen (WMD 0.61 mg/g freeze-dried feces; 95% CI: - 0.35 - 1.57) in a random effects model (p < 0.01, χ2 test; I2 = 86.0%). When those studies were divided by lesion (cancer vs. adenoma) in order to explain the heterogeneity existed, the heterogeneity existed. In a random effects model, patients with large bowel cancer had a non significant higher concentration of total bile acids (WMD 0.43 mg/g freeze-dried feces; 95% CI: - 0.83 - 1.69) (p < 0.1, χ2 test; I2 = 88.5%) (Fig. 2). Under fixed effects model, the fecal excretion of total bile acids was significantly higher in patients with adenoma than in controls (WMD 0.66 mg/g freeze-dried feces; 95% CI: 0.08 - 1.24), but this difference was no longer significant when based on random effects models (WMD 1.13 mg/g freeze-dried feces; 95% CI: - 0.25 - 2.51).
Individual bile acid
CDCA
Five studies reported the relationship between CDCA and cancer/adenoma of the large bowel. No heterogeneity existed about CDCA (p > 0.1, χ2 test; I2 = 33.7%). Significantly increased concentration of CDCA was seen by a fixed effects model when all studies were pooled to assess the relationship between CDCA and cancer/adenoma of the large bowel (WMD 0.13 mg/g freeze-dried feces; 95% CI: 0.01 - 0.25). The fecal excretion of CDCA was significantly higher in patients with large bowel cancer than in matched controls (WMD 0.28 mg/g freeze-dried feces, 95% CI: 0.10 - 0.46) in a fixed effects model (Fig. 3), and also with random effects models (WMD 0.28 mg/g freeze-dried feces; 95% CI: 0.09 - 0.48). However, no differences existed between patients with adenoma and controls (WMD 0.00 mg/g freeze-dried feces; 95% CI: - 0.17 - 0.17) by a fixed/random effects model.
DCA
All studies were pooled to assess the relationship between fecal DCA and cancer/adenoma of the large bowel. DCA excretion in patients with cancer/adenoma was not significantly different compared to corresponding controls (WMD 0.24 mg/g freeze-dried feces; 95% CI: - 0.43 - 0.91; random effects model). DCA excretion in patients with cancer was significantly different compared to corresponding controls under fixed effects models (WMD 0.33 mg/g freeze-dried feces; 95% CI: 0.10 - 0.57) (Fig. 4), but the significance was lost with random effects models (WMD 0.01 mg/g freeze-dried feces; 95% CI: - 0.86 - 0.88). However, statistical heterogeneity was present (p < 0.01, χ2 test; I2 = 89.2%). DCA excretion in patients with adenoma on admission was significantly higher than in patients with corresponding controls under fixed effects models (WMD 0.69 mg/g freeze-dried feces; 95% CI: 0.18 - 1.20). There was no heterogeneity existed (p > 0.01, χ2 test; I2 = 56.1%).
Lithocholic acid
LCA excretion in patients with cancer was significantly higher than in patients with corresponding controls under fixed effects models (WMD 0.30 mg/g freeze-dried feces; 95% CI: 0.07 - 0.52) (Fig. 5), and no significance exists between patients with adenoma and patients with corresponding controls. All studies were pooled to assess the relationship between fecal LCA and cancer/adenoma of the large bowel. LCA excretion in patients with cancer/adenoma was nonsignificantly higher than in patients with corresponding controls (WMD 0.61 mg/g freeze-dried feces; 95% CI: - 0.03 - 1.24) under random effects model.
Sum of primary and secondary bile acids
Primary bile acids in patients with cancer/adenoma were slightly higher than in patients with matched controls, but little differences were seen (WMD 0.20 mg/g freeze-dried feces; 95% CI: - 0.10 - 0.51) (random effects model) (Fig. 6). For secondary bile acids, no significance was seen between patients with cancer and patients with matched controls regardless of fixed and random effects models (Fig. 7).
Sub-analysis / sensitivity analysis
For sub analysis, we calculated the WMD and 95% CI by geographical location. In Europe, there was no difference between patients with cancer/adenoma and patients with matched controls. However, total bile acids excretion in patients with cancer/adenoma was slightly higher than in patients with matched controls in Asia, although no significance was seen. There was only 1 study investigating the relationship in North America that showed significantly higher level of total bile acids in patients with cancer/adenoma compared to matched controls. In the sensitivity analysis, we excluded the studies conducted by Meance et al.,17 which contained probiotics in the diet. The concentration of total bile acids had no significant changes.
Publication bias
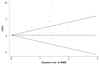
For total bile acids excretion, no evidence of publication bias was observed as indicated by a symmetric funnel plot and a non-significant Begg test (p = 0.47) and Egger test (p = 0.23) (Fig. 8).
DISCUSSION
Colorectal cancer is the third most common cancer in both men and women, and is the second leading cause of cancer deaths.27 Investigators have identified several risk factors that increase a person's chance of developing colorectal cancer, such as age, diet, large intestinal polyps, family history of colon cancer, medical conditions, lack of exercise, obesity, diabetes, smoking, familial adenomatous polyposis, Gardner's syndrome, etc.28 Among these risk factors, observational evidence to relate fecal bile acids and risk of colorectal cancer/adenoma is abundant, however, these studies reported contradictory conclusions.
Therefore, we performed a meta-analysis of all eligible studies in order to address the relationship between FBAs and colorectal cancer or adenoma. The time-related analysis also suggested that FBA concentrations are not an important risk factor for carcinoma unless they are greater than 9 mg/g of feces.21 The finding of this analysis suggests no association between total FBAs and cancer/adenoma of the large bowel, regardless of being based on fixed (WMD 0.14 mg/g freeze-dried feces; 95% CI: - 0.19 - 0.47) and random effects models (WMD 0.61 mg/g freeze-dried feces; 95% CI: - 0.35 - 1.57). However, there was significant heterogeneity (p < 0.01, χ2 test; I2 = 86.0%). Adjustment for clinically relevant confounders in these studies makes this possibility less likely but does not completely eliminate it. Our meta-analysis also showed that the fecal excretion of CDCA was significantly higher in patients with cancer/adenoma than in controls (WMD 0.13 mg/g freeze-dried feces; 95% CI: 0.01 - 0.25), especially for colorectal cancer (WMD 0.28 mg/g freeze-dried feces; 95% CI: 0.10 - 0.46). However, no differences existed between patients with adenoma and controls (WMD 0.00 mg/g freeze-dried feces; 95% CI: - 0.17 - 0.17). In vivo, CDCA markedly enhanced tumor growth and increased vascularization via the COX-2 pathway.29
Animal model experiments indicate that DCA and LCA act as colon tumor promoters of an established large bowel animal carcinogen.30,31 For fecal excretion of DCA and LCA, significantly increased concentrations of DCA and LCA were seen under fixed effects models [(WMD 0.40 mg/g freeze-dried feces; 95% CI: 0.18 - 0.61) and (WMD 0.32 mg/g freeze-dried feces; 95% CI: 0.12 - 0.53), respectively]. However, the significance was lost with random effects models [(WMD 0.24 mg/g freeze-dried feces; 95% CI: - 0.43 - 0.91) and (WMD 0.61 mg/g freeze-dried feces; 95% CI: - 0.03 - 1.24), respectively]. There was also significant heterogeneity. For the sum of primary and secondary bile acids, no significances were seen although there was no heterogeneity. Secondary bile acids have been found to be mutagenic and promote tumor growth in animal models, and the feces of populations with a low risk of colonic cancer contain relatively low proportions of secondary bile acids.32 Furthermore, it has been shown that the proportion of secondary bile acids, namely LCA and DCA, is a far better marker for colorectal cancer.
LCAs and DCAs are the product of 7α-dehydroxylation of CDCA and cholic acids. Cholic acid is mainly derived from endogenous cholesterol whereas CDCA is synthesized mainly from dietary cholesterol.33,34 Some studies demonstrated that Americans who consume a mixed Western diet are, a high risk population and excreted high levels of bile acids compared to Japanese, Chinese, and American Seventh-Day Adventists, who are at low risk.35,36 We purposed that diet patterns have a definite influence upon bile acids metabolism.
Furthermore, many studies also reported the ratio of LCA/DCA, and suggested that the ratio of LCA/DCA may be an important discriminant marker for susceptibility to colorectal cancer.37 The LCA/DCA ratio was significantly higher in the colorectal cancer group compared to the control group.14 Another interesting feature has emerged from some studies that relate the LCA/DCA ratio to the excretion of total FBAs, LCA/DCA×FBA index showing a positive correlation with colorectal cancer.12
Many factors may contribute to the discrepancy in results of observational studies. Firstly, wide variations in the excretion of bile acids in feces have been reported between individuals and from day-to-day within the same individual. Variations in bile acid metabolism might mainly be influenced by age, transmit time, hepatic function, liver metastases, use of medication, gall bladder function, and undergoing previous cholecystectomy and bowel surgery. Secondly, methodological aspects including selection of subjects, period of feces collection, and chemical analysis of either total feces are of great influence. Thirdly, FBA profiles are complex because of bacterial deconjugation, dehydroxylation, oxidoreduction, and desulphation of bile acids in the intestine.
This meta-analysis has several strengths and limitations. Although funnel plot and formal testing did not indicate publication bias, bias cannot definitely be ruled out because of the small number of studies and the low power of any test to detect publication bias. There was evidence of heterogeneity concerning the outcomes of total bile acids, DCA, and LCA. Adjustment for clinically relevant confounders in these studies makes this possibility less likely but does not completely eliminate it. One limitation of our study is the lack of data from multiple large trials. Furthermore, to some extent, the techniques used for FBA determination, which represent little advance since their development in the mid 1960s, can be criticized for lacking in specificity and being incapable of detecting trace quantities of the types of compounds proposed as carcinogens or cocarcinogens. Furthermore, the definition of the sum of secondary bile acids is different; some studies included DCA and LCA which others included DCA, LCA, and ursodeoxycholic acid. Nevertheless, the detailed composition of the sum of primary bile acids in each study is consistent.
In conclusion, by showing differences between the bile acid profiles of patients with colorectal adenomas or carcinomas and matched controls, we provided further support for the concept that bile acids have a role to play in the development of large bowel tumors. The present findings also raise possibility that the biochemical analysis of fecal CDCA might be useful in screening populations for high and low risk in developing carcinoma of the colon.






 XML Download
XML Download