

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Tuberculosis is a pandemic and highly contagious disease. Of 6.1 billion world population, 2 billion people, which are approximately one-third of the entire population, have been infected with Mycobactericum tuberculosis, and 1% of the population is being introduced as carriers every year. Of these carriers, 7 - 8 million people develop tuberculosis and 2 million die of the disease.1 In Korea, the incidence of tuberculosis was 72.1 in 100,000 in the year 2001, decreased to 67.2 in 2002, 64.0 in 2003, and then slightly increased to 65.4 in 2004.2 Death from tuberculosis in Korea was 6.7 in 100,000 in the year 2001, 7.0 in 2002, and 6.9 in 2003.3
Due to the world wide increase in the incidences of immune-related diseases such as acquired immunodeficiency syndrome (AIDS), the incidence of tuberculosis is also being increased. In that context, Korea is no exception, therefore more prompt and accurate diagnosis of tuberculosis is required.4
Diagnosis of tuberculosis consists of signs and symptoms, X-ray findings, and detection of M. tuberculosis. Currently, bacterial culture, AFS, and PCR are employed to isolate M. tuberculosis. Bacterial culture method is feasible only if > 100 M. tuberculosis are present in 1 mL of specimen. Although the specificity of the culture method is close to 100% so as to be used for final diagnosis, 3 - 8 weeks are required to cultivate the bacteria. The culture method is also not cost efficient.5-8 AFS is a relatively fast simple procedure and cost efficient. Nevertheless, it needs 5,000 - 10,000 bacteria present in 1 mL of sample and does not discriminate M. tuberculosis against other non-tuberculosis mycobacteria, leading to low sensitivity (22 - 78%).5-8 PCR detects M. tuberculosis directly in the specimen and does not require weeks-long incubation time so as to be fit for early diagnosis. The disadvantage of PCR method is that it detects not only viable M. tuberculosis but non-viable M. tuberculosis. Thus, the method is not used for definitive diagnosis.5,9-11 Moreover, variations in diagnostic procedures and specimens lead to different rate of specificity between different labs.12-20
Given the above mentioned information, this study was designed to evaluate in-house PCR method by comparing it with conventional AFS, bacterial culture method, and commonly used Cobas Amplicor M. tuberculosis™ kit (Roche Molecular System, Inc., Branchburg, NJ, USA).
MATERIALS AND METHODS
Patients
In this study, we retrospectively analyzed the results of in-house PCR, AFS, and culture for tuberculosis diagnosis in 2,973 patients who visited Kyung Hee Medical Center between July 2003 and July 2006. We also compared 29 in-house PCR positive and 91 in-house PCR negative cases (total 120 cases) between April 2006 and July 2006 with commercially available Cobas Amplicor M. tuberculosis™ kit, AFS, and culture.
Specimens
Sputum, bronchial aspirate, pleural fluid, urine, cerebrospinal fluid, tissue, and other body fluid were analyzed. Sputum, bronchial aspirate, urine, and pus were incubated for 15 minutes at room temperature in 4% NaOH and then centrifuged for 15 - 20 minutes at 3000 g. Tissues were minced with scissors, to which 1 mL of K buffer and 300 µg/mL proteinase K were added and incubated for 3 hours at 55℃. After heating for 10 minutes at 95℃ and centrifugation for 5 minutes at 7000g, 2 µL of supernatant were collected and analyzed. Cerebrospinal and other body fluid were centrifuged without any pretreatmet.
AFS
Fluorochrome-stain positive specimens were Ziehl-Neelsen stained and the results were then determined under 1,000 × magnification with > 300 field according to classification of the Center for Disease Control.21
Culture of Mycobacterium tuberculosis
Specimens were inoculated onto 3% Ogawa media and then incubated for at least 8 weeks at 37℃. Specimens were observed once every week.
In-house PCR
Samples were collected in Tris ethylenediaminetetraacetic acid (EDTA) [10 mM Tris-HCl ([H 8.0], 1 mM EDTA), centrifuged twice at 7000 rpm for 5 minutes. After discarding supernatant, samples were heated for 10 minutes in 5% Chelex 50 - 200 µL and Tris EDTA buffer and centrifuged at 12,000 rpm for 5 minutes. Two µL of supernatant was added to 20 µL of reaction mixture [14 µL sterilized water, 2 µL PCR buffer, 3.0 mM MgCl2, 0.8 µL 2.5 mM deoxynucleoside triphosphate (Core Biosystem, Seoul, Korea), loading dye 1 µL, Taq DNA polymerase (Core Biosystem, Seoul, Korea) 0.1 µL 1.0 µL primers (Bioneer, Daejeon, Korea)] and amplified (GeneAmp PCR system 9600; Perkin-Elmer Medical Instruments, CT, USA) with 30 cycles at 94℃ for 20 seconds, 60℃ for 20 seconds, and 72℃ for 30 seconds. Primer sequences are shown in Table 1. Two µL of 10 times-diluted PCR product was again amplified with the same condition at the first PCR. PCR product (285 bp) was checked for size by comparing positive M. tuberculosis using 2% agarose gel electrophoresis. To minimize cross-contamination, DNA extraction and amplification were performed in separate rooms.
Cobas Amplicor M. tuberculosis™
DNA extraction and amplification were performed according to the manufacturer's instructions.
Diagnosis of tuberculosis
Tuberculosis was diagnosed when culture was positive. Culture negative tuberculosis was also diagnosed based on positive results of other diagnostic methods such as AFS and PCR. In addition, clinical signs, X-ray and hemological findings, and responses to anti-tuberculosis drugs were also considered.7,8,22 Culture-positive non-tuberculosis Mycobacterium was excluded.
RESULTS
Analysis of in-house PCR, AFS, and culture
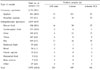
Of 2,973 samples, pulmonary samples were 1,134 (38.1%) [sputum 864 (29.0%), bronchial aspirates 271 (9.1%)] non-pulmonary samples were 1,839 (61.9%) of which pleural fluid was 834 (28.1%) (Table 2). Of pulmonary samples, 212 (18.7%) were positive for in-house PCR, 80 (7.1%) for AFS, and 129 (11.4%) for culture. Of non-pulmonary samples, 79 (4.3%) were positive for in-house PCR, 40 (2.2%) for AFS, and 67 (3.6%) for culture (Table 2). Of 2,973, 244 cases (8.2%) were diagnosed as tuberculosis, 112 of which were consistently positive for AFS, culture, and PCR (Table 3). Of 132 cases that displayed inconsistent results in AFS, culture, and PCR, 123 were finally diagnosed as tuberculosis and the remaining 9 were diagnosed as pneumonia (2), bronchiectasia (2), chronic obstructive pulmonary diseases (2), esophageal cancer (1), peripartum infection (1), and bronchitis (1). The 9 cases were all positive for in-house PCR (Table 4). The sensitivities for in-house PCR, AFS, and culture were 77.5%, 49.2%, and 80.7%, respectively, and specificities were 99.7%, 100%, and 100%, respectively (Table 5).
Analysis of in-house PCR and Cobas Amplicor M. tuberculosis™ kit
Of 120 samples, pulmonary samples were 81 (67.5%) and non-pulmonary samples were 39 (32.5%). Of pulmonary samples, 17 (21.0%) were positive for in-house PCR and 20 (24.7%) for Cobas Amplicor™. Of non-pulmonary samples, 10 (25.6%) were positive for in-house PCR and 3 (7.7%) for Cobas Amplicor™ (Table 6). Nineteen cases were consistently positive in both in-house PCR and Cobas Amplicor™, and 3 were consistently negative. Inconsistent results were found in 10 cases, of which 9 (3 sputum samples positive for Cobas Amplicor™ and 2 pleural fluid, 2 urine, and 2 tissue samples positive for in-house PCR) were diagnosed as tuberculosis and 1 as chronic obstructive pulmonary disease (1 sputum sample weakly positive for in-house PCR). The sensitivities of in-house PCR and Cobas Amplicor™ were 81.3% and 71.9%, respectively (pulmonary samples, 77.3% and 90.9%. non-pulmonary samples, 90.0% and 30.0%, respectively) (Table 7).
DISCUSSION
Diagnosis of tuberculosis usually includes clinical symptoms, X-ray findings, and detection of M. tuberculosis. To detect M. tuberculosis in clinical samples, laboratory employs AFS, culture of M. tuberculosis, and PCR. AFS is fast but the sensitivity is low whereas culture of M. tuberculosis needs long turnover time but sensitivity and specificity are high. PCR assay, the sensitivity and specificity of which are high and widely used in many clinical laboratories, requires only very small amounts of M. tuberculosis to diagnose tuberculosis.
In a study by 6 laboratories AFS, culture, and PCR were analyzed, and the pooled sensitivities were found to be 55.5%, 89.3%, 85.2%, respectively, and pooled specificity was 99.7% for all 3 diagnostic methods.22 Our study showed that the sensitivities for AFS, culture, and PCR were 49.2%, 80.7%, 77.5%, respectively, and specificities were 100%, 100%, and 99.7%, respectively, indicating lower sensitivity and higher specificity. Another study demonstrated that the sensitivities for AFS, culture, and PCR were 41.3%, 65.7%, and 59%, respectively, which are lower than those in our study and the specificities > 97%, and also demonstrated that PCR in combination with AFS increased sensitivity up to 65%, which is similar to that of culture method, suggesting the possibility for standard diagnostic procedure for tuberculosis.7 Given the high sensitivity and specificity of PCR method, we suggest that PCR is very useful for the diagnosis of tuberculosis, except when drug sensitivity and detection of non-tuberculosis mycobacteria are required. PCR may be used in AFB smear-positive samples for final diagnosis of tuberculosis.8
Nine false-positive results were found with in-house PCR in this study. Two were pneumonia, 2 bronchiectasia, 2 chronic obstructive pulmonary diseases, 1 esophageal cancer, 1 peripartum infection and 1 bronchitis. False positive may be caused by the contamination of amplicons.9,23-25 The contamination is even higher in in-house PCR, which requires multiple steps of specimen processing procedures than in commercial kit.23 False positive may also be caused by the fact that PCR can not distinguish between viable and non-viable M. tuberculosis.9,23-25
Fifty-five cases in this study were found to be false negative. False negative may be caused by the presence of inhibitors, loss of M. tuberculosis during DNA extraction procedures, and amplification methods.9,25 Since this is a retrospective study, determination of the causes of false-positive and false-negative results is limited.
The sensitivity and specificity estimates for in-house PCR vary widely, ranging from 63 - 100% for the sensitivity and 62 - 100% for the specificity.5,26-34 The difference in the sensitivity of PCR may be due to analytical sensitivity of PCR, PCR assay shows difference in sensitivity depending on the target of PCR and whether it is nested PCR or not. In particular, high sensitivity was obtained when IS6110 was the target. In addition, the distribution of positive samples in the specimen, especially in weak positive samples,5 affects the sensitivity of PCR, particularly contamination by amplicon.34
In this study, the sensitivity and specificity were 81.3% and 98.9% in in-house PCR and 71.9% and 100% in Cobas Amplicor M. tuberculosis™ kit, indicating higher sensitivity and lower specificity in in-house PCR. Intriguingly, when samples were subdivided into pulmonary and non-pulmonary, non-pulmonary samples showed lower sensitivity (30%) than pulmonary samples (Table 7). This result is not in line with a study in which diagnostic results of in-house PCR and Cobas Amplicor M. tuberculosis™ kit in pulmonary and non-pulmonary samples were analyzed.20 The reason of why inconsistent results were observed in our study could be due to the fact that the amount of specimens was inadequate or specimens were weakly positive for M. tuberculosis.35
Another study in which diagnostic results of in-house PCR and Cobas Amplicor M. tuberculosis™ were analyzed demonstrated sensitivities of 91.08% and 66.33% for in-house PCR and Cobas Amplicor M. tuberculosis™ kit and specificities of 99.85% and 99.71%,35 which are similar to our results. Lower sensitivity in Cobas Amplicor M. tuberculosis™ kit may be attributed to the use of single copy and ELISA or smaller amount of sample (0.1 mL in Cobas Amplicor™ and 1.0 mL in in-house PCR). The possibility that lower sensitivitiy in Cobas Amplicor M. tuberculosis™ kit may be due to the presence of inhibitors has also been suggested.36
Our laboratory employed nested PCR that requires 2 rounds of amplification procedure and confirmed PCR products not by Southern blotting but agarose gel electrophoresis. Thus, different primers, the amount of samples, and amplification method might have affected sensitivity. As demonstrated by the manufacturer, Cobas Amplicor™ displayed significantly lower sensitivity in nonpulmonary samples and higher sensitivity in pulmonary samples than in-house PCR (p < 0.01). More samples and further followup are required for in-depth study, nevertheless we suggest that Cobas Amplicor™ is a useful and time-efficient diagnostic method.
In summary, despite the high false-positive diagnostic results, we demonstrated that in-house PCR at Kyung Hee Medical Center can be used in place of AFS and culture for the early diagnosis of tuberculosis. Furthermore, in-house PCR showed higher sensitivity in non-pulmonary samples than Cobas Amplicor™ kit. Cobas Amplicor™ kit is time efficient and has the advantage of lower false-positive rates in the diagnosis of tuberculosis.





 XML Download
XML Download