

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Ischemic colitis results from the same conditions that cause hypoperfusion or embolic/thrombotic occlusion of the vascular supply of the colon.1 Many factors may be involved in the hypoperfusive state that results in ischemic colitis. Nonocclusive ischemia is now a well-recognized condition, though its pathophysiology is still not completely understood.2 Vasoconstrictive medications may be implicated in some cases of nonocclusive ischemia. These medications include digitalis, diuretics, estrogen, cocaine, pseudoephedrine, methamphetamine, vasopressin, alosetron, and non-steroidal anti-inflammatory drugs.1,2
Ephedra sinica or ma huang is an evergreen shrub native to Central Asia, and its primary component is ephedrine.3 Food supplements containing ephedra alkaloids have been linked to adverse cardiovascular and central nervous events.4 Additionally, a case of ischemic colitis associated with the use of an herbal product was reported in a young woman.5 In this paper, we examine the strong association between the use of ma huang and the development of ischemic colitis.
CASE REPORT
A 40-year-old man was admitted to our emergency department with abdominal pain and bloody diarrhea. The patient had watery diarrhea for 3 days, but 3 hours prior to presentation, it became bloody. He had neither a history of symptoms suggestive of an inflammatory bowel disease nor a recent history of antibiotic use. In addition, he had neither a history of recent travel nor a diet change. His medical history was unremarkable for risk factors of bowel ischemia, except for hypertension that was well controlled with angiotensin receptor blockers. He smoked 1 pack of cigarette per day for 10 years, and there was no family history of cerebrovascular or cardivascular disease. Notably, he had been taking an herbal food supplement, Ephedra sinica or ma huang (total 1,000 mg; 3 times/day) throughout the previous month for weight loss.
His blood pressure was 110/70 mmHg, pulse rate 73/min, respiratory rate 20/min, and body temperature 36.5℃. His body mass index was 25.7 kg/m2. The patient appeared acutely ill but otherwise was a healthy, well-nourished man. His abdomen was soft and obese with mild tenderness in the periumbilical area, and his bowel sounds were normoactive. Laboratory data on admission showed hemoglobin 15.6 g/dL, hematocrit 44.4%, white blood cell count 7,500/mm3, and platelet 214,000/mm3. His serum sodium level was 138 mmol/L, potassium 4.1 mmol/L, chloride 103 mmol/L, fasting glucose 98 mg/dL, serum albumin 3.9 g/dL, total cholesterol 145 mg/dL, triglyceride 75 mg/dL, LDL cholesterol 81 mg/dL, blood urea nitrogen 10 mg/dL, and creatinine 1.2 mg/dL. The patient's coagulation profiles were normal. The stool white blood cell test was negative, while the stool occult blood test was positive. Stool specimens were negative for enteric pathogens.
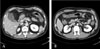
Abdominal and pelvic CT scans showed a patent superior mesenteric artery and circumferential wall thickening of the ascending, transverse, and descending colon sparing the rectosigmoid junction (Fig. 1). Colonoscopy performed on admission showed findings compatible with segmental colitis extending from the ascending to the descending colon. The involved areas were edematous and hyperemic, with areas of frank hemorrhage (Fig. 2A). Three days after intravenous hydration and nutritional support, the bloody diarrhea resolved. At an 8-day follow-up, colonoscopy showed markedly improved mucosa without any complications (Fig. 2B). The colonoscopic biopsy specimen of the affected area showed focal mucosal erosion and chronic inflammatory cell infiltration consistent with ischemic colitis (Fig. 3).
The patient completely recovered without complications and with only conservative management. On discharge, he was advised to discontinue the use of herbal medications and to avoid any ephedrine- or pseudoephedrine-containing cold remedies.
DISCUSSION
Herbal weight loss supplements are popular and may even be effective. Ma huang is a source of ephedrine, a long-acting sympathomimetic that acts primarily through the release of stored catecholamine via α- and β-adrenoreceptors.5 Ephedra and ephedrine are sometimes used to achieve weight loss or to enhance athletic performance, but the efficacy and safety of these compounds are uncertain.6 Moreover, during the past decade, a considerable number of reports regarding the adverse effects of ephedra have led to an increased awareness of the danger of these sympathomimetics. For example, herbal ephedra and ephedrine-containing food supplements have been reported to increase the risks of adverse psychiatric, autonomic, and gastrointestinal events.6 Furthermore, ephedrine and related alkaloids have been associated with adverse cardiovascular events, including acute myocardial infarction, severe hypertension, myocarditis, and lethal cardiac arrhythmia.7-9 Ephedrine can also predispose patients to both hemorrhagic and ischemic stroke.10
Ephedrine and ephedra are found to promote short-term weight loss in clinical trials, but no data are available regarding long-term weight loss.6 A recent study found that products containing ephedra accounted for 64% of all adverse reactions to herbal supplements reported to the US poison control centers in 2001, even though they accounted for only 1% of the herbal supplement market.11 Although a number of clinical trials have reported adverse events associated with Ephedria sinica,12-14 information regarding the supplement is still incomplete. Ma huang is considered to be potentially safe by the Food and Drug Administration (FDA) when used orally for a maximum of 7 days and in maximum doses of 24 mg/day of ephedrine equivalent.15 However, in light of recently reported adverse events, the FDA has proposed limits on the dose and duration of these supplements.4 In this case, the patient was taking ma huang in a dose about 6 times higher than is recommended by the FDA. It is not surprising, therefore, that ischemic colitis developed in this patient. Infectious etiologies were also ruled out with stool analysis.
Injury to the colon, especially ischemic colitis, in patients using ma huang is presumably related to reduced splanchnic blood flow due to vasoconstrictions such as those seen in myocardial infarction8 and ischemic stroke.10 Potentially at-risk areas include sites in the splenic flexure, descending colon, and occasionally the rectosigmoid junction. The areas between the superior and inferior mesenteric arteries and between the lower sigmoid and superior rectal arteries are known as 'watershed' areas.5
Recently, a few cases of ischemic colitis have been reported to be linked with decongestant use.16-17 In each of these cases, the vasoconstrictive properties of pseudoephedrine were believed to be the possible cause of ischemic colitis. Moreover, ischemic colitis after a dietary supplementation with phenteramine, an amphetamine-derived sympathomimetic, has been reported.18 Although our patient did not take decongestant medications, his herbal diet supplements contained ephedrine products, which were similar to pseudoephedrine and caffeine products.12-14
It is important to keep in mind that many healthy people take a variety of herbal medications, believing that these medications are completely harmless. However, herbal products have many active ingredients with pharmacologic properties that may have undesirable effects. This paper suggests that use of ma huang, a known sympathomimetic and vasoconstrictor, carries a risk for ischemic colitis in healthy people.


 XML Download
XML Download