

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Solitary fibrous tumor (SFT) is a spindle cell neoplasm of assumed mesenchymal fibroblastic origin.1 It was originally described in the thoracic visceral pleura, but has since been reported in extrathoracic sites such as the meninges,2 liver,3 and tunica vaginalis testis.4 Recently, spinal cord and nerve involvement has also been reported.5-8 We report a rare case of SFT mimicking a dumbbell-shaped cervical spinal cord tumor, which had MRI findings different from those in previous reports.6,9,10
CASE REPORT
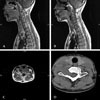
A 40-year-old Asian female presented with a 2-month history of right shoulder pain and Grade 4 right triceps weakness. Sensory examination revealed no abnormalities. Deep tendon reflexes were hypoactive at the right triceps and normoactive at both knee joints. Evidence of myelopathy was absent. Magnetic resonance imaging (MRI) revealed an extramedullary, extradural, dumbbell-shaped spinal cord tumor at the level of C6-C7 (Fig. 1A, B and C). A computerized tomographic (CT) scan revealed a dumbbell shaped mass and enlarged neural foramen at the level of C6-C7 (Fig. 1D). The tumor measured 5.5cm along its long axis. There was low signal intensity on T2-weighted images, iso-signal intensity on T1-weighted images, and homogenous enhancement by gadolinium. The preoperative impression was schwannoma. Through a midline cervical incision, muscle was bilaterally retracted, and the lower C6 and upper C7 lamina sections and the medial part of the right C6-7 articular joint were removed. The tumor was firmly adhered to the C6-7 neural foramen, and attachments to the right C7 nerve were noted. Excision was performed through a T-shaped incision on the dura and nerve root using a sonic aspirator, with special caution at the nerve root. Gross total resection was accomplished with sparing of the nerves; the tumor was found to have a rubbery consistency and was relatively avascular. The patient's postoperative course was uneventful and her posterior neck pain disappeared. There was no neurological compromise, except mild hypoesthesia of the right middle finger. Histological examination revealed monomorphous spindle cells with a storiform pattern (Fig. 2A), and many areas of perivascular hyalinization. Necrosis and mitoses were absent. Immunohistochemistry was positive for CD34 and CD99 and negative for epithelial membrane antigen (EMA), smooth muscle acting (SMA), and S100 (Fig. 2B). Histological and immunohistochemical findings were consistent with SFT.
DISCUSSION
A solitary fibrous tumor is a spindle cell tumor that was first described in the thoracic visceral pleura, but also found in multiple extrathoracic sites, including the meninges,2 liver,3 and tunica vaginalis testis.4 SFT may originate from a unique, perivascular multipotent mesenchyme that shares a lineage with pericytes, fibroblasts, and infrequently, endothelium.1 Consequently, morphological features of SFT may be varied with constituent cells that are predominantly undifferentiated, pericytic, or fibroblastic in nature.1 It has recently been reported that SFT involves both intra- and extramedullary portions of the spinal cord.5-8 Therefore, SFT arising in the spinal cord should be differentiated from schwannoma, meningioma, hemangiopericytoma, and hemangioblastoma.5-9 Clinical and radiological differentiation are not possible. Usual MRI findings included hypointensity on T1- and T2 weighted imaging, reflecting fibrous tissue;6,9,10 however, in our case, isointensity on T1 and hypointensity on T2-weighted imaging were noted. Hemangioblastoma could be ruled out by intraoperative findings.9 Although morphological features are helpful, such as alternating Antoni A and Antoni B areas in schwannoma and cellular whorls and psammoma bodies in meningioma, immunohistochemical findings are essential.7 Schwannomas are invariably S-100 protein positive and meningiomas are epithelial membrane antigen positive, whereas both antibodies are absent in SFT. In addition, SFT is characteristically positive for CD34, bcl-2, and vimentin, but negative for GFAP, neuron specific enolase, and cytokeratin.9 Hemangiopericytoma is CD34 positive in 50%, but dense collagen bands are usually absent.7 Because local recurrence and malignant transformation have been reported, long-term follow up is mandatory.1,2,11,12 Radiation therapy for remnant SFT is not recommended.6 In our case, gross total resection was accomplished, and there was no evidence of mitoses and necrosis; yearly follow-up was scheduled. At 8 months postoperatively, there was no evidence of tumor recurrence.
In our case, the tumor was exposed and removed with resection of the medial right C6-7 articular joint half; however, complete removal of a unilateral articular joint may be necessary for large dumbbell-shaped tumors of the cervical spinal cord. In such cases, posterior cervical fusion may be needed to prevent iatrogenic cervical kyphosis and neck pain.13
In conclusion, SFT should be included in the differential diagnoses of spinal cord tumors, especially those that show spindle cell lesions. Most importantly, long term follow-up is necessary due to clinical uncertainty.

 XML Download
XML Download