

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Bronchopulmonary dysplasia (BPD), a form of chronic lung disease usually occurring in premature infants, is an important cause of mortality and morbidity during the neonatal period with few effective treatment.1 Histopathologic characteristics of BPD include airway injury, inflammation, and parenchymal fibrosis.2-4 The precise mechanism of BPD has not yet been elucidated, therefore, it was felt of necessity to better understand its pathophysiologic mechanism to develop therapeutic modality that can prevent lung injury and consequently improve the prognosis of BPD.
Clinically, antenatal inflammation, diagnosed by chorioamnionitis or by elevated cytokines in amniotic fluid, is associated with increased risks of preterm delivery and BPD.5 Neonatal sepsis and/or pneumonia also are known to be risk factors of BPD.6 However, chorioamnionitis has been associated with decreased incidence of respiratory distress syndrome7 and improved survival.8 In experimental animals, lung inflammation can be produced by administering endotoxin, a lipopolysaccharide component of Gram-negative bacteria.9,10 Intra-alveolar inflammatory cell recruitment and/or reduced alveolar growth were observed after intratracheal11 or intraamniotic endotoxin administration.12 However, systemic administration of endotoxin significantly protected lungs against oxygen toxicity in neonatal rats.13 Therefore, available data on the role of inflammation due to infection in the development of BPD remain dubious, and further studies are needed to clarify this. This study was done to determine the effects of intratracheal administration of endotoxin on hyperoxia-induced lung injury in neonatal rats.
MATERIALS AND METHODS
Animals and study design
The experimental protocols described herein were reviewed and approved by the Animal Care and Use Committee of the Samsung Biomedical Research Institute in Seoul, Korea. This study also followed the institutional and National Institutes of Health guidelines for laboratory animal care. Timed pregnant Sprague Dawley rats were housed in individual cages with free access to water and laboratory chow, and pups were delivered spontaneously. The experiment began within 12 hours after birth and was continued through postnatal day 14.
Rat pups were divided into four experimental groups: normoxia control group (NC, n=21), normoxia with endotoxin treatment group (NE, n=24), hyperoxia control group (HC, n=46), and hyperoxia with endotoxin treatment group (HE, n=48). Throughout the experiment, rat pups of NC and NE were kept in standard cages with nursing mother rat at room air, and pups of HC and HE were kept in standard cages with mother rat within 50 liter Plexiglas chamber in which hyperoxia (> 95% oxygen concentration) was maintained. Humidity was maintained at 50%, and environmental temperature was maintained at 22-24℃. To avoid oxygen toxicity of nursing mother rat, mother rats were rotated daily between litters in normoxia groups and hyperoxia groups.
Pups in NE and HE were injected with E. coli endotoxin (0.5µg in 0.03mL, Lipopolysaccharide, LPS from Escherichia coli O55:B5; Sigma, St Louis, Mo; 10mg) intratracheally at the 1st, 3rd and 5th postnatal day. Rats were restrained on a board on a fixed angle, neck was palpated to locate the trachea, and 1cc syringe with a 30-gauge needle was introduced into the trachea for instillation of endotoxin. Intratracheal location of the needle was confirmed by withdrawal of air into the syringe with minimal reflux of suspension back through the nose. Air was pulsed after each liquid volume. Pups in NC and HC received an equal volume of normal saline administered in the same way. Animals were returned to their dams after the procedure, and there was no mortality associated with the procedure.
Survival and body weight of rat pups in each group were checked daily throughout the experiment, and were sacrificed at postnatal day 14 after intraperitoneal injection of ketamine (Yuhan Corp., Seoul, Korea, 50mg/kg).
Tissue preparation
After perfusion of the heart with normal saline, lungs were fixed in situ at a constant inflation pressure of 20cm H2O and fixed overnight in 10% buffered formalin. The fixed lung tissue was embedded in paraffin wax after tissue processing. Five µm-thick sections were cut from the paraffin block and stained with hematoxylin and eosin. Images of each section were captured with Baumer optronic digital camera through an Olympus BX40 microscope (Olympus optical co. Ltd., Tokyo, Japan) and were saved as JPEG files.
Lung histopathology
Alveolarization was assessed by performing radial alveolar counts (RAC), according to the method of Emery and Mithal.14,15 From the center of the respiratory bronchiole, a perpendicular line was drawn to the edge of the acinus (as defined by a connective tissue septum or the pleura), and the number of the septa intersected by this line was counted.
The intra-alveolar distance was measured as the mean linear intercept (MLI), obtained by dividing the total length of lines drawn across the lung section by the number of intercepts encountered, as described by Cooney and Thurlbeck.16 After obtaining the RAC and MLI values, the RAC/MLI ratio was calculated in each case.
Each successive lung field was individually assessed for severity of interstitial fibrosis and allotted a score 0 and 8, as described by Ashcroft et al.17 A minimum of 10 lung fields per section was examined for each analysis.
Statistical analyses
All data are presented as mean±standard deviation. Statistical comparison between each group was performed by one-way analysis of variance with Bonferroni's correction. For comparison of survival curves, Kaplan-Meiyer analysis was performed. A p-value of < 0.05 was considered significant.
RESULTS
Mortality and body weight gain
At the end of the experiment (postnatal day 14), exposure to oxygen groups significantly decreased the survival rate (HC and HE, 48% and 58%, respectively) compared to normoxia groups (NC and NE, 89% and 75%, respectively) (Fig. 1).
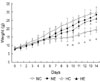
Although birth weights were not different between the four experimental groups, pups nursed in hyperoxia alone (HC) showed significant decrease in body weight compared to normoxia groups (NC, NE) after postnatal day 7, and this hyperoxia-induced decrease of body weight was improved with endotoxin administration (Fig. 2).
Lung histopathology
Representative photomicrographs showing histopathologic differences in each experimental group are shown in Fig. 3. Morphometric analyses revealed slight but significant decrease in RAC and RAC/MLI ratio and increased fibrosis score in NE compared to NC (Fig. 4, 5). Compared to normoxia groups (NC, NE), RAC and RAC/MLI ratio in HC were significantly decreased, whereas MLI and fibrosis score were significantly increased. These hyperoxia-induced lung morphometric abnormalities, however, were significantly attenuated with endotoxin administration (HE).
DISCUSSION
The development of an appropriate animal model that can simulate clinical BPD of premature infants is essential for delineation of its pathophysiologic mechanism. The saccular stage of the newly born rat pup corresponds to the lung developmental stage of premature infants at 25-28 weeks gestation18 and alveolarization occurs during the first 2 weeks after birth.19 Hence, the newborn rat pup model is a model very suitable for studying pathophysiologic mechanisms of BPD. In the histopathologic study of the lung, Husain et al.20 reported that RAC, MLI, and their ratios are simple and the most useful way of studying acinar growth and development.
Oxidative stress to the immature lung is a well-known risk factor for the development of BPD.21-23 In the present study, prolonged exposure of newborn rat pups to hyperoxia developed lung injuries similar to those seen in human infants with BPD,2 exhibiting decreased alveolarization as evidenced by decreased RAC, increased MLI3 and markedly increased fibrosis.4
Mild arrest in alveolar growth that was evidenced by a slight decrease in the RAC and RAC/MLI ratio, and an increase in fibrosis was also observed in the endotoxin treated normoxia group (NE) compared to NC. These findings strengthen the assumption that inflammation due to infection can disrupt alveolar development in preterm lung, causing histological changes similar to BPD.12,13,24,25 However, endotoxin administration during hyperoxia (HE) significantly attenuated hyperoxia-induced abnormalities, such as an increase in MLI and fibrosis score, decrease in RAC, RAC/MLI ratio, and body weight. Taken together, our data indicate that the friend or foe simple dichotomy could not account for the complex role of inflammation induced by endotoxin in the pathogenesis of BPD.
Although hyperoxia-induced mortality in the present study was not significantly improved, growth retardation observed in HC was significantly attenuated with endotoxin treatment (HE). Growth retardation observed in HC might be attributable to higher caloric requirements of rat pups with more severe lung disease. More severe pathologic findings and clinical symptoms of BPD, such as dyspnea and tachypnea, in HC than in HE support our speculation.
The precise mechanisms by which endotoxin attenuates hyperoxia-induced lung injury are not completely understood. The protective effects of endotoxin might be attributable to a combination of enhanced lung maturation,26,27 increased antioxidants,13,28 surfactant,12,29,30,31 loss of L-selectin and reduced neutrophils in the lung,32 and increased anti-inflammatory cytokines such as interleukin 11 and 13.33
Significant attenuation of the hyperoxia-induced lung injury with endotoxin treatment observed in this study contradicts the results by Kohno et al. who reported that the most remarkable emphysematous changes were noted in endotoxin plus hyperoxia group.34 As 10-week old rats were used in the above study compared to 1-day-old newborn rat pups in this study, differences in the stage of lung maturation might be responsible for these discrepancies with endotoxin treatment.
In the present study, endotoxin was given intratracheally. Since the protective effect has also been observed against the hyperoxia-induced lung injury with systemic (intraperitoneal) administration of endotoxin,13 the protective effects of endotoxin appear to be not influenced by the routes of administration.
Despite such effects of endotoxin, low survival rate was noted in HC and HE groups on day 14 of the study, and this could be explained by relatively high death rate in the endotoxin-administered groups (NE and HE) during the earlier study period. It is highly likely that the concentration of endotoxin was higher than that used in earlier studies, and that there was some leakage into the systemic circulation.
The results described herein led us to conclude that the administration of endotoxin, a potent proinflammatory mediator, significantly attenuated hyperoxia-induced neonatal lung injury as evidenced by improvement in the arrest of alveolarization and in the increased fibrosis. These findings do not support the assumption that antenatal inflammation due to infection causes BPD, instead suggesting some beneficial effects of chorioamnionitis.




 XML Download
XML Download