

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
The thoracolumbar junction (TLJ) is the transition zone between the thoracic spine and the lumbar spine.1,2 The spinal cord transitions to the cauda equina in the TLJ, which contains the upper and lower motor neurons of the spinal cord and the cauda equina.1,2 As a result, clinical features of lesions in the TLJ vary,1,2 and anatomical characteristics may affect surgical outcome. Spinal cord tumors (SCTs) are an uncommon cause of lower back pain and radiating leg pain.3 Previous reports indicate that clinical features of SCTs of the TLJ are similar to those of intervertebral disc diseases (IVDs).4,5 A computerized tomographic (CT) scan is inferior in discriminating the contents of the spinal canal.6 CT scans for patients with lower back pain and radiating leg pain are usually performed around the L3-4-5-S1 intervertebral spaces.4 In some cases, magnetic resonance imaging (MRI) scans of the lumbar spine omit the TLJ. Consequently, SCT of the TLJ can be missed. This study was conducted to investigate the characteristic clinical features and surgical outcomes of SCTs of the TLJ. We excluded SCTs of the cauda equina because they are relatively well recognized and easily detected with routine lumbar MRI.7 The TLJ is anatomically defined as the region from the T12 to L1 vertebrae.1 For our purposes, however, the TLJ was defined as the region from T11 to L2, due to individual variation in the presence of the T12 vertebra and the location of the caudal end of the spinal cord.
MATERIALS AND METHODS
A retrospective review was performed of 76 patients surgically treated at our institute for SCTs arising from T11 to L2 between 1998 and 2006. Pathological diagnosis, clinical features, neurological signs, and surgical outcomes were investigated using medical records and imaging studies. There were 45 males and 31 females. The mean age was 48 years, with a range from 11 to 82 years. The mean follow-up period was 40 months, with a range from 1 to 68 months. MRIs were taken in all patients before and after surgery. The caudal end of the spinal cord was determined from sagittal and axial images on the MRI. The caudal end of the spinal cord was located between the lower half of the body of L1 and the upper half of the body of L2 in all patients. The patients were divided into two groups: epiconus (affected levels T11-T12, n-18) and conus (affected levels L1-L2, n = 58). If a tumor involved both T12 and L1, classification was based on the more involved side. Patients with multiple SCTs and solitary SCTs exceeding the TLJ were excluded. If the patient had multiple symptoms, the most severe symptom was regarded as the presenting symptom. All patients were examined and operated upon by the corresponding author (YDH).
All patients underwent tumor resection after laminotomy. The laminotomy was as wide as necessary to sufficiently expose both the cranial and the caudal ends of the tumors. The dura was incised and retracted laterally. Complete excision was attempted in most cases. However, when the tumors adhered strongly to the spinal cord or the cauda equina, these were incompletely removed to preserve neurological function. The tumors were internally decompressed using an ultrasonic aspirator, then excised (except for vascular tumors). The resected lamina was reattached to the vertebra to prevent postoperative kyphosis and skin dimpling.
Chi-square analysis was used to evaluate differences between the epiconus and conus groups. p values of < 0.05 were considered statistically significant.
RESULTS
SCTs of the TLJ
During the study period, 419 SCTs were surgically treated at our institute; SCTs of the TLJ accounted for 18% of all SCTs. The affected levels were the epiconus (T11-T12) in 18 patients and the conus (L1-2) in 58 patients. There were 58 intradural-extramedullary tumors (76%) with 2 paraspinal extensions, 17 intramedullary tumors (22%), and 1 epidural tumor (1%). The pathological diagnoses were as follows: 51 schwannomas (67%, cellular type: 2), 8 ependymomas (11%, cellular type: 7, myxopapillary type: 1), 4 lipomas, 3 meningiomas (meningothelial type: 2, pasmmomatous type: 1), 2 hemangioblastomas, 2 astrocytomas, 2 cavernous angiomas, 2 metastases (with 1 intramedullary metastasis from lung cancer and 1 intradural-extramedullary metastasis from brain glioblastoma), and 2 neurofibromas (summarized in Table 1). The pathological entity did not vary between the two groups.
Clinical features
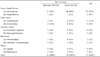
Deep tendon reflex (DTR) was normoactive in 40 patients (53%), hypoactive in 21 patients (28%), and hyperactive in 15 patients (20%) (Table 2). The epiconus group had more hyperactive DTRs, while the conus group had more normoactive and hypoactive DTRs. The patterns of DTR were statistically different between the two groups (p < 0.01, Table 3). Nerve tension signs, including the femoral nerve stretching test (FNST) and the straight leg raising test (SLRT), were positive in 24 patients. Nerve tension signs were more frequently observed in the conus group (p < 0.05, Table 2).
Duration between the onset time of initial symptoms and the time of correct diagnosis was less than 6 months in 41 patients (54%) and more than 6 months in 35 patients (46%); the average duration was 10 months. Of the patients whose correct diagnosis was delayed by more than 6 months, 9 (26%) were misdiagnosed as IVDs. In addition, four patients (5%) received both tumor removal and lumbar discectomy due to comorbid IVDs (Fig. 1).
Surgical outcomes
Complete excision was achieved in 68 patients (89%). Incomplete excision was inevitably achieved in eight patients due to adhesion to the spinal cord or nerve root (n = 6) or an ill-defined border of an intramedullary SCT (n = 2). The presenting symptoms improved in 69 patients (91%), remained unchanged in four patients (5%), and worsened in 3 patients (4%). The data are summarized in Table 3. In the three patients with worsening symptoms, two showed severe adhesion to the spinal cord and the cauda equina and one had an intramedullary diffuse astrocytoma with an ill-defined border. Surgical complications included dysesthesia in 10 patients (13%), neurogenic bladder in seven patients (9%), paraparesis in three patients (4%), and CSF leakage in two patients (3%). Of the 22 patients with surgical complications, 14 patients (64%) improved spontaneously.
DISCUSSION
SCTs of the TLJ
SCTs make up 15% of all central nervous system neoplasms.8 In the present study, SCTs of the TLJ made up 18% of all spinal cord tumors surgically treated at our institute. Patients with nerve sheath tumors and glial tumors constituted almost 83% of the sample. Nerve sheath tumors accounted for 70% of the sample, and schwannoma was the most common pathology. Glial tumors accounted for 10% of the sample, and ependymoma was the most common intramedullary pathology. It is known that astrocytomas in the conus and cauda equina make up less than 4% of all spinal cord astrocytomas, but one half of spinal cord ependymomas are found in this region.9 In our study, ependymomas were four times more common than astrocytomas and were more frequent in the conus group. The high concentration of ependymal cells around the region of the filum terminale is thought to be one cause of the high frequency of ependymomas in the TLJ.10
Clinical features
Early recognition of SCTs of the TLJ (before they give rise to irreversible neurological sequelae) remains the most important challenge.7,11 Early diagnosis is important for reducing surgical invasion and aiding adequate recovery from symptoms, but is often disturbed.3-5,12 More than half (61%) of the sample reported pain as the presenting symptom, with leg pain appearing more frequently than back pain in both groups. Nerve tension signs (including FNST and SLRT) were observed in 32% of the sample. Nerve tension signs were more commonly seen in the conus group. It is known that myelopathy is generally preceded by leg pain and back pain.4 The L4, L5, and S1 nerve roots emerge at the level of the T10 vertebra and descend to lower levels.4 The nerve roots may be compressed by tumors at both the epiconus and the conus. The nerve roots are more crowded at the conus, however, and the chance of nerve root irritation by the tumor increases. In this study, DTRs were more hyperactive in the epiconus group and hypoactive in the conus group, probably because the upper motor neurons are located in the epiconus and the lower motor neurons are located in the conus.1 Though there were differences in both groups, the distinction was of little clinical value.10 In addition, it is important to note that differentiation of SCTs of the TLJ from other conditions (such as IVDs) is difficult when based only on clinical features.4,5,7,13 Symptomatic similarities may cause diagnostic delays of four months to three years in conus and cauda equina tumors. In nearly half of the sample, it took more than six months for a correct diagnosis to be made. Nine patients were misdiagnosed as IVDs and had received physical therapy for a long time. It was impossible in the four patients who had both SCTs and IVDs to definitively determine the exact cause of their symptoms. Both the size of the SCT and protruded intervertebral disc were significantly large in three patients. One patient had a long history of upper back pain and recently aggravated leg pain, and both symptoms exceeded 6 in the visual analog scale. Consequently, these patients underwent combined surgeries for both pathologies.
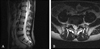
CT scans are inferior in discriminating the contents of the spinal canal.4,14 CT scans for patients with lower back pain and radiating leg pain are usually performed at L3-4-5-S1 intervertebral spaces.4,14 A 27-year-old female patient had a CT scan for chronic back and leg pain, but her CT scan was performed at the L2-3-4-5-S1 intervertebral spaces and early diagnosis failed (Fig. 2). A cavernous angioma was diagnosed after it had bled (Fig. 2). At times, MRIs of the lumbar spine omit the TLJ.
Surgical outcomes
In most cases, complete excision was achieved and surgical outcomes were favorable. The causes of incomplete excision were adhesion to the spinal cord or nerve root and an ill-defined border of an intramedullary spinal cord tumor. It is generally agreed that preservation of neurological function is more important than complete excision by force.3
In conclusion, among SCTs of the TLJ, the epiconus group displayed upper motor neuron syndrome, and the conus group displayed lower motor neuron syndrome. SCTs of the TLJ were frequently misdiagnosed as IVDs due to their symptomatic similarities. SCTs of the TLJ should be included in differential diagnosis of back and leg pain, and it is highly recommended that routine lumbar MRI include the TLJ.



 XML Download
XML Download