

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Scimitar vein is a serious anomaly because the partial anomalous pulmonary venous connections usually drain the right lower lobe of the lung to the inferior vena cava and inevitably cause cyanosis. Scimitar vein is often associated with congenital bronchopulmonary vascular malformations and is uncommonly presented as an isolated anomaly. Clinical manifestations in patients with isolated scimitar vein anomalies may be subtle and diagnosis can only be achieved after scrupulous identification. In contrast, the patients with complex cardiovascular and bronchopulmonary malformations, the clinical or radiological stigmata of scimitar vein anomalies could be overlooked by the overwhelming manifestations of congestive heart failure, pulmonary hypertension, and pneumonia. Clinical discrimination between isolated scimitar vein anomalies and complex scimitar vein anomalies associated with cardiopulmonary malformations is crucial for the outcomes vary. In this article, we report the clinical features, diagnosis, and discrimination of isolated and complex scimitar vein anomalies and differentiate these cases from cases with the meandering right pulmonary vein reported in the literature.
MATERIALS AND METHODS
From January 1990 to December 2006, 4 female patients (aged 2 days to 3.5 years) were studied retrospectively. One patient had the adult form (or isolated scimitar vein anomaly) and 3 patients had the infantile form of the scimitar vein anomalies (or scimitar vein complex with other congenital cardiovascular and bronchopulmonary malformations). Study modalities, including profile recordings of the clinical features (n = 4), plain chest radiographs (n = 4), Doppler echocardiography (n = 4), cardiac catheterization with angiography (n = 4), magnetic resonance imaging (n = 3), surgery (n = 2), computer tomography (n = 1), bronchography (n = 1), magnetic resonance angiography (n = 1), and autopsy (n = 1) were reviewed to support the diagnosis.
Illustrated cases
Scimitar vein anomaly with complex malformations, infantile onset, infantile form
Patient 1 was a 2-month-old female infant. She presented with tachycardia, tachypnea, lip cyanosis (oxygen saturation of 80%), dextroversion of the heart, and lobar pneumonia of the right lower lobe due to a classical triad of the scimitar syndrome: (1) bronchopulmonary sequestration of the right lower lobe, (2) a systemic arterial supply from the thoracic aorta to the right lower lobe, and (3) anomalous drainage of the right lower pulmonary vein to the inferior vena cava as a right-handed scimitar vein. Because the pulmonary venous drainage was not dual in character, surgical removal of the right lower lobe together with ligations of the systemic feeding artery and the anomalous pulmonary draining vein were indicated and performed successfully. This patient was free of congestive heart failure and recurrent pneumonia since the surgical correction.
Patient 2 was an 8-month-old female infant. She presented with tachycardia (atrial flutter), dyspnea, cardiomegaly, hepatomegaly, pneumonia, and lip cyanosis (oxygen saturation of 67%) due to a constellation of dextrocardia, heterotaxy, right atrial isomerism, common atrium, common atrioventricular valve, d-loop dominant right ventricle, double outlet right ventricle, dextro-malposition of the great arteries (aorta is located right-anterior to main pulmonary artery), infundibular pulmonary stenosis (pressure gradient of 63 mmHg), a left-sided PDA from the left aortic arch, juxtaductal coarctation of the left pulmonary artery, bilateral superior vena cava, left-sided inferior vena cava, and anomalous pulmonary venous connections. The right middle and the right lower pulmonary veins drained into the hepatic vein as a right-sided scimitar vein. The left pulmonary veins drained to the left venoatrial junction (left superior vena cava and the left-sided right atrium) and the right upper pulmonary vein drained to the right venoatrial junction (right superior vena cava and the right-sided right atrium). This patient did not survive the palliative bilateral Glenn's shunts.
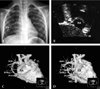
Patient 3, who presented with remarkablecyanosis (oxygen saturation of 50%), tachycardia, tachypnea, and hepatomegaly in the 4th day of life, had a fascinating complex of bronchial solitus with bronchial stenosis, midline liver, heterotaxy, dextrocardia, right atrial isomerism, common atrium, common atrioventricular valve, single ventricle, pulmonary atresia, total anomalous pulmonary venous connection to the left hepatic vein, a left-sided scimitar vein (a left-handed sword) (Figs. 1A and B), total anomalous hepatic venous connection, bilateral superior vena cava, interruption of the inferior vena cava with azygos vein continuation to the right superior vena cava, and bronchopulmonary sequestration. This patient died of sepsis in spite of surgical construction of a patent systemic-to-pulmonary central shunt.
Isolated scimitar vein anomaly, beyond infantile onset, adult form
Patient 4 was referred from the pediatric infection clinic due to recurrent infection of lung at the age of 3.5 years old. Upon examination, this patient looked pink and her oxygen saturation exceeded 96% on the peripheral pulse oximeter. In addition, the physical examination found that she had fine moist rales over the right lung fields and a soft systolic ejection murmur of grade 1/6 over the left upper sternal border. In spite of medical treatment, the plain chest film constantly showed loss of cardiac silhouette at the lower right cardiac border together with a positive scimitar sign (Fig. 2A). Echocardiography showed an anomalous vessel connecting the right atrium (Fig. 2B). Cardiac catheterization with angiography was performed to discriminate the discrepancy between clinical absence of cyanosis and radiological positive scimitar signs. The latter condition is suggestive of partial anomalous pulmonary venous connection. Serendipitously, we found no desaturation of oxygen in the left ventricle or in the aorta (99%). In contrast, oxygen saturations in the right atrium, in the right ventricle, and in the pulmonary artery were 85%, while oxygen saturation in the inferior vena cava and the superior vena cava were 78% and 75%, respectively. The ratio of pulmonary blood flow to systemic blood flow was 1.7. In the levophase of the main pulmonary arteriography, two abnormal vessels could be visualized to drain the lower right atrium above the diaphragm. Oxygen saturations in these two vessels, which could be probed and entered through the right atrium, were 99%. Chest computer tomography (General Electric, Lightspeed Ultra 16, WI, USA) documented a scimitar vein above the diaphragm (Figs. 2C and D), yet without the other two stigmata of scimitar syndrome, namely, an anomaly of the bronchopulmonary airways with systemic arterial supplies to the incriminated segment or lobe of the lung. For treatment, this isolated scimitar vein anomaly, which was camouflaged by a dual system of pulmonary venous drainage of the right lung, was approached transvenously and occluded successfully by the Amplatzer Ductal Occluder (ADO) (AGA Medical Corporation, Golden Valley, MN, USA) when the patient was 4 years old. At the 6-month follow-up, chest radiographs showed ADO in situ of the scimitar vein. Echocardiography with color Doppler showed complete occlusion of the scimitar vein. These devices did not migrate or protrude into the right atrium. Neither intracardiac vegetation, nor massive pulmonary thromboembolism was noted. At the 12-month follow-up, cardiac catheterization with angiography showed normalization of the oxygen saturation in the right atrium, normalization of the pulmonary arterial pressure, complete occlusion of the scimitar vein, and normal pulmonary venous drainage to the left atrium without obstruction. After interventional cardiac catheterization, neither arrhythmia, nor recurrent pneumonia was observed. The recurrent pneumonia in this patient may be caused by a significant left-to-right shunt (or pulmonary overflow) producing increased wetness and decreased ventilation of her right lung.
RESULTS
Table 1 contains the tabulated clinical profiles of 4 patients with isolated scimitar vein anomalies and complex scimitar vein anomalies with the congenital cardiovascular and bronchopulmonary malformations. These 4 patients were female with ages ranging between 2 days to 3.5 years. The salient clinical features were recurrent lung infection in all 4 patients, acute respiratory distress, congestive heart failure, pulmonary hypertension, and/or cyanosis in 3 patients, dextrocardia, complex congenital cardiovascular malformations, heterotaxy, and/or right atrial isomerism in 2 patients, as well as dextroversion, right bronchial isomerism, bronchial stenosis, and sepsis in 1 patient. Patients 2 and 3 had complex congenital cardiovascular malformations (dextrocardia, right atrial isomerism, common atrium, common atrioventricular valve, double outlet ventricle, pulmonary atresia, and heterotaxy) and bronchopulmonary malformations (right bronchial isomerism in both patients and bronchopulmonary sequestration in patient 3). Radiographic scimitar signs could be identified in all 4 patients. A left-sided scimitar vein anomaly, i.e., a left-handed sword, was noted in the patient 3. Patients 1, 2, and 3 had early onset congestive heart failure, pulmonary hypertension, pneumonia, and cyanosis. Patient 4 caught our attention only after the patient suffering from a recurrent pneumonia that was refractory to medical care together with a persistent loss of silhouette at the right lower cardiac border on the plain chest radiographs.
DISCUSSION
The scimitar etceteras and their unscrupulous nomenclatures require a new naming system, such as pseudo-scimitar syndrome, incomplete scimitar syndrome, scimitar variant, scimitar vein syndrome, and even meandering right pulmonary vein as a scimitar variant.
First, the scimitar syndrome, the scimitar vein, and the scimitar sign must be defined precisely to avoid inaccurately attributing one for the others. Cooper and Chassinat, who did not use the word "scimitar syndrome" or "scimitar" in their papers, reported in 1836 individually rare congenital malformations that involved venous drainage "below" the diaphragm.1,2 The words of "scimitar" and "scimitar syndrome" appeared in the literature in 1956 and 1960,3,4 respectively. Since that time, there has been no consensus on the precise definition of scimitar syndrome. However, we could derive three major features from these two pioneer reports, namely, the anomalous pulmonary venous connection to the inferior vena cava (scimitar vein), a systemic arterial supply to the right lung, and bronchial anomalies of the hypoplastic right lung.3,4 The so-called bronchial anomalies of the hypoplastic right lung may include bronchial diverticulum,3 bronchial hypoplasia or stenosis,3 and abnormal branching of the bronchial trees.4 Another two features of less constancy merit our discussion. Midline shifting of the heart in dextroposition (rather than dextrocardia) is a secondary effect due to hypoplasia of the right lung and should not be included as a criterion for defining scimitar syndrome. In scimitar syndrome, the systemic artery could supply either a segment or a lobe of a normal lung,4 an abnormal lung without bronchopulmonary sequestration,3 or an abnormal lung with bronchopulmonary sequestration.5-7 Neither the dextroposed heart, nor bronchopulmonary sequestration is a sine qua non criterion for defining scimitar syndrome.
Second, the scimitar vein shall be preserved exclusively to denote anomalous pulmonary vein draining part or all of the right lung into the inferior vena cava or into its junction with the right atrium. We deem that the scimitar vein is both eponymous and exclusive to scimitar syndrome. The scimitar vein anomaly is the most irreplaceable characteristic of scimitar syndrome. Thus, this characteristic shall be maintained as a major criterion for defining scimitar syndrome. However, it is indiscriminate to implicate scimitar sign on the plain chest film to be scimitar vein, to which pseudo-scimitar syndrome was serendipitously attributed. The scimitar sign only refers to the curvilinear picture of the frontal chest film that mimics a scimitar (a curved Turkish sword). It should not be taken for granted that the presence of a scimitar sign implies the presence of a scimitar vein (anomalous pulmonary venous connection to the inferior vena cava), and vice versa, because these radiographic findings could be false positive8-11 or false negative12,13 in predicting presence of the scimitar vein (anomalous pulmonary venous connection to the inferior vena cava). Although the presence of a scimitar sign shall prompt us to search for the scimitar vein, neither the scimitar sign, nor the scimitar vein, nor the occurrence of both will fulfill the aforementioned diagnostic criteria for scimitar syndrome. It is amiss to state that the diagnosis of scimitar syndrome should be expanded and based solely on a distinct scimitar sign (rather than a true scimitar vein) on chest radiographs.11 Although a scimitar sign in a female patient with normal pulmonary venous connections may be called a pseudo-scimitar syndrome,9 it was an imprecise and unscrupulous nomenclature. In the literature, we found reports of so-called scimitar vein syndrome,13 scimitar variant,14,15 and incomplete scimitar syndrome.16 None of these 4 reports documented any systemic arterial supply or anomaly of the bronchial airway.13-16 Therefore, the patients in these reports were victims with the isolated scimitar vein anomaly.
Third, a congenital horseshoe lung could be associated with the scimitar vein,17-19 or without the scimitar vein,17 and vice versa. The congenital horseshoe lung has two pertinent pathologic findings, including branching anomalies of the bronchial airway and the pulmonary artery. In cases of the congenital horseshoe lung, we must go further into cardiac catheterization and angiography to identify a scimitar vein, a systemic arterial supply, and a pulmonary artery branching anomaly to make a diagnosis of scimitar syndrome. In a report describing 3 patients with the crossover lung segment,20 all were victims of congenital horseshoe lung with scimitar syndrome. Contrarily, in patients with a radiographic scimitar sign or angiographic scimitar vein, congenital horseshoe lungs should be identified prudently.
Fourth, a meandering right pulmonary vein (MRPV) was the last straw. MRPV has been coined by Goodman as an anomalous right pulmonary vein that courses circuitously through the right lung, silhouetted as scimitar sign on the chest radiograph, and drains into the left atrium.21 MRPV is another condition that could be inappropriately labeled as scimitar variant and even scimitar syndrome, especially when the scimitar vein is not prudently identified. However, not all patients with MRPV have scimitar signs, scimitar veins, or the full-fledged stigmata of scimitar syndrome. Though we found reports of MRPV with8,9,11,21,22 and without scimitar syndrome,23-27 only the patient reported by Tortoriello had scimitar syndrome.22 We recommend that MRPV should be preserved to describe the right pulmonary vein coursing circuitously within the right lung, but draining normally to the left atrium. Thus, MRPV will not cause cyanosis hemodynamically. Patients with partial anomalous pulmonary venous drainage to the inferior vena cava or the right atrium should be regarded as having a scimitar vein anomaly. In observance of these two criteria, the patients reported in the following 18 reports8,9,11,13-16,21-31 could have the revised diagnosis from isolated MRPV8,9,21,23-26 to MRPV with bronchopulmonary sequestration,11 and from isolated scimitar vein anomalies with dual pulmonary venous drainage (to the inferior vena cava and the left atrium)14,15,23,27,28 to isolated scimitar vein anomalies without dual pulmonary venous drainage13,16,29-31 and scimitar syndrome.22 A total of 22 cases with scimitar vein anomalies, and 8 cases with MRPV were tabulated and compared in Table 2.
Finally, the Amplatzer Ductal Occluder (ADO) (AGA Medical Corporation, Golden Valley, MN, USA) has been proved to be an effective vehicle for occluding a non-isolated scimitar vein anomaly with dual pulmonary venous drainage, an aortopulmonary collateral artery from the abdominal aorta to the right lower lobe,32 and an isolated scimitar vein anomaly with dual pulmonary venous drainage.33 Our decision to use ADO to occlude the isolated scimitar vein anomaly in this case was based on the scenarios that the pulmonary venous drainage of the right lung was dual in character, no associated cardiovascular or bronchopulmonary malformations requiring surgery, the transvenous approach was easily feasible, the devices could be deployed outside the cardiac chambers, the retention skirt of the ADO could be appropriately profiled to counter the current of the centripetal pulmonary venous flow to the right atrium, and open chest surgery and prolonged hospitalization could be obviated.33 We present the first documented case of an isolated scimitar vein anomaly, which was camouflaged by dual pulmonary venous connections of the right lung, and treated successfully with a catheter-base device of ADO.33
In conclusion, the clinical pictures and radiological stigmata of the scimitar vein anomaly could be overlooked because of the overwhelming heart failure and pulmonary hypertension in a complex infantile form.34 For patients with isolated scimitar vein anomalies, the clinical symptoms and signs may be subtle and a diagnosis can be made only after a scrupulous assessment.35 Discrimination of the underlying pathology and the clinical features of scimitar vein anomalies is crucial for the outcomes vary.



 XML Download
XML Download