

 ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Aneurysm of the sinus of Valsalva (SVA) is a rare clinical manifestation of Behçet's syndrome. Only a few cases of SVA accompanying Behçet's syndrome have been reported.1-3 Since the SVAs caused by an active inflammatory disease, such as Behçet's syndrome, tend to enlarge progressively and have a high risk of rupture, early diagnosis and surgical management is critical for the patient survival.
CASE REPORT
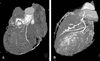
A 45-year-old female was admitted to the emergency department for intermittent chest pain, which had been aggravated 30 minutes before admission. She had been suffering from recurrent oral and genital ulcers and had been diagnosed with Behçet's syndrome for two years. She was taking oral medications, including Colchicine. Upon physical examination, her blood pressure was 118/70mmHg, and her pulse rate was 71 beats/min. A 12-lead EKG revealed a normal sinus rhythm with nonspecific ST & T-wave abnormalities. Initial laboratory findings showed increased total creatinine phosphokinase (CPK) of 94IU/L and an MB fraction of 8.7ng/mL (0.0-5.0ng/mL). C-reactive protein (CRP), one of the acute phase reactants, was also elevated to 53mg/L (reference range 0.0-8.0mg/L). A transesophageal echocardiogram (TEE) revealed mild aortic regurgitation and normal ventricular wall motion. A coronary angiogram showed an 80% luminal narrowing of the proximal to middle left anterior descending artery and a 70% stenosis of the first diagonal branch. Since coronary artery disease subsequent from Behçet's disease was suspected, we planned elective coronary artery bypass grafting (CABG) and started medical treatment with intravenous heparin and isosorbide dinitrate, along with corticosteroids, to control Behçet's disease activity while also monitoring the patient's CRP. After two weeks of medication with steroids, the CRP was normalized, but the patient complained of more frequent chest pain. Suspecting the progression of coronary artery disease, we performed a non-invasive, multi-dimensional computed tomogram (MD-CT). MD-CT revealed a dilated left SVA with a huge aneurysm compressing the proximal left anterior descending artery and the left circumflex artery (Fig. 1A). Since the aneurysm was huge and the patient complained of severe chest pain, an emergent operation was performed. Intraoperative TEE showed regional wall motion abnormality of the anterolateral segment, and EKG monitoring showed ST elevation. The operation was performed through a median sternotomy with mild hypothermic cardiopulmonary bypass. The aorta was cross-clamped and opened transversely. The orifice of the aneurysm was observed at the left SVA. The size of the orifice was about 2cm in diameter, and it originated about 5mm from the left main coronary ostium. The orifice, filled with organized mural thrombi (Fig. 2A), was closed with a two-layered autologous pericardium and a Dacron patch, and the CABG was performed between the left anterior descending and the obtuse marginal coronary arteries, using left internal mammary and radial artery composite Y-grafts. Since the left coronary cusp of the aortic valve was fibrotic and retracted into the left ventricular outflow tract, aortic valvuloplasty was performed concomitantly (Fig. 2B). The patient was weaned from cardiopulmonary bypass uneventfully, and intraoperative TEE revealed improved anterolateral wall motion and trivial aortic regurgitation. A postoperative MD-CT, performed one month after surgery, showed patent bypass grafts with a regressed aneurysm (Fig. 1B). The patient was followed-up for nine months, and recovery has been uneventful.
DISCUSSION
An SVA is a rare cardiac anomaly that is observed in only 0.14-0.96% of open-heart surgeries.4 Most SVAs are congenital, and acquired SVAs are rare. Acquired SVAs can be caused by a deficiency of the aortic media, which may result from trauma, endocarditis, syphilis, connective tissue diseases, such as Marfan's syndrome or Behçet's syndrome, or a senile type of dilation.5
Behçet's syndrome is a systemic inflammatory disease with rare cardiac and vascular manifestations, such as pericarditis, aortic or mitral regurgitation, endomyocardial fibrosis, arterial or venous occlusion, and varices and aneurysms of the sinus of Valsalva, which can occur in about five percent of patients.1,6 Both SVAs and Behçet's syndrome occur more frequently in Asian patient populations.1,7
In our case, although Behçet's syndrome is diagnosed only with clinical manifestations, SVA was considered to be caused by Behçet's syndrome since the disease progression was too rapid and initial laboratory findings revealed an elevated CRP which was normalized with steroid treatment. Before surgery, our patient showed compromised cardiac function, caused by aneurysmal compression of the left coronary system. Since the huge SVA was filled with organized thrombi and it was not feasible to resect and remove the SVA completely, we closed the orifice with a patch and reestablished coronary circulation with bypass grafts; cardiac function improved, and the patient became symptom-free after surgery. Although advances in echocardiography have reduced the need for other diagnostic procedures, we could not detect the SVA in the initial TTE since it was too small at that time. The MD-CT taken after two weeks showed a huge SVA, which suggested a rapid progression of the disease.
Although unruptured SVAs are mostly asymptomatic, fatal complications, such as infection, systemic embolism, right ventricular outflow tract obstruction, malignant arrhythmias, and acute coronary syndrome, can occur.8 In addition, SVAs caused by active inflammatory disease, such as Behçet's syndrome, tend to enlarge progressively and have a high risk of rupture, early surgical repair may reduce mortality and morbidity.

 XML Download
XML Download