

 ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Nontuberculous mycobacteria (NTM) are ubiquitous organisms, increasingly recognized as an important cause of chronic pulmonary infection in non-immunocompromised individuals.1 Among NTM, the Mycobacterium avium complex (MAC) and M. abscessus constitute the most commonly encountered agents of NTM lung disease in Korea.2-4
Mycobacterium xenopi is a slow-growing NTM. The prevalence of M. xenopi varies geographically; it is one of the most commonly isolated NTMs in the United Kingdom,5 France,6 and Canada.7 In contrast, it is less commonly identified in the U.S.1 M. xenopi is a very rare pathogen of pulmonary disease in Asia. Until recently, only eight cases of M. xenopi pulmonary disease have been reported in Japan.8
Here, we describe a case of M. xenopi pulmonary disease, the first reported in Korea. The isolates were identified, using both conventional microbiological methods and heat-shock protein 65 gene (hsp65) sequence analysis.
CASE REPORT
A 66-year-old man with no history of smoking was referred to our hospital for further examination and management of probable NTM lung disease. His history was significant for pulmonary tuberculosis 44 years earlier, for which he underwent right upper lobectomy to palliate recurrent hemoptysis.
Two months before admission to our hospital, the patient reported a 2-month history of productive cough, hemoptysis, and mild fever. He also experienced 10kg weight loss, associated with a poor appetite. Chest X-ray demonstrated cavitary consolidation in the right lung, and an acid-fast bacilli (AFB) stain was positive in his sputum (2+). The patient was initially diagnosed with pulmonary tuberculosis and received isoniazid, rifampicin, ethambutol, and pyrazinamide. After two months of anti-tuberculous treatment, during which the patient failed to improve clinically, he was transferred to our hospital.
Physical examination upon presentation showed that the patient was 172cm tall and weighed 54kg. Vitals included a body temperature of 37.5℃ and a respiratory rate of 20 breaths/min. Coarse crackles over the right hemithorax were revealed upon auscultation. No lymphadenopathy was appreciated.
Laboratory tests revealed a white blood cell count of 10,520/µL, with a differential of 84.7% neutrophils. The erythrocyte sedimentation rate was 120mm/h, and the level of C-reactive protein was elevated at 16.55mg/dL. Total proteins were 7.0g/dL, with a low albumin level (2.3g/dL). A human immunodeficiency virus antibody test was negative.
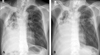
Chest radiograph revealed a huge cavitary consolidation involving the entire right lung (Fig. 1A). Significant AFBs were visualized in multiple sputum specimens; however, repeated nucleic acid amplification tests for M. tuberculosis, using a commercial DNA probe (Gen-Probe Amplified Mycobacterium Tuberculosis Direct Test; Gen-Probe Inc, San Diego, CA, USA) were negative. Combination chemotherapy, which included clarithromycin (1000mg/day), rifampicin (600mg/day), ethambutol (800mg/day), and streptomycin (750mg intramuscular injection three times per week), was initiated under the tentative diagnosis of MAC disease.
Subsequently, more than five isolates of mycobacteria, obtained from sputum specimens at both hospitals, were transferred to the Korean Institute of Tuberculosis and Department of Microbiology and Immunology at the College of Medicine of Seoul National University. Species isolation was performed, using both conventional microbiological and molecular methods.9,10 All isolates were identified as M. xenopi, based on heat-shock protein 65 gene (hsp65) sequence analysis, showing 100% sequence similarity with the M. xenopi reference strains (Fig. 2). Other mycobacteria were not isolated along with M. xenopi. The isolates from this patient were sensitive to isoniazid (0.2 µg/mL), rifampicin (40 µg/mL), streptomycin (4 µg/mL), and kanamycin (40 µg/mL); but were resistant to ethambutol (2.0 µg/mL) on Lowenstein-Jensen media. The isolates were also susceptible to clarithromycin (16 µg/mL), rifabutin (2 µg/mL), amikacin (16 µg/mL), and moxifloxacin (1 µg/mL) in Middlebrook7H9 broth.
Despite four months of antibiotic therapy, the disease was progressive. The patient suffered from profound sputum production and hemoptysis. A chest X-ray revealed that the size of the right lung cavitary consolidation had increased, and a new infiltrative shadow appeared in the left lung (Fig. 1B). The patient complained of decreased hearing, leading to a discontinuation of streptomycin treatment. In light of disease progression and the side effects of streptomycin, the patient was re-admitted to the hospital whereupon moxifloxacin (400mg/day) was added to the treatment. The patient's condition improved slightly; however, he eventually underwent right completion pneumonectomy. Pathology specimens revealed a near-totally destroyed lung and severe necrotizing granulomatous inflammation with caseating necrosis. Postoperatively, gradual improvements of the clinical features and radiologic findings were observed, and a negative conversion of sputum examinations was achieved. However, a late bronchopleural fistula developed acutely 47 days postoperatively, and the patient subsequently expired with pneumonia and respiratory failure.
DISCUSSION
To the best of our knowledge, this is the first case of pulmonary disease caused by Mycobacterium xenopi in Korea. M. xenopi was clearly shown to be the etiologic agent of the cavitary consolidative changes in our case. Considering clinical and radiographic features, in addition to repeated isolation of M. xenopi, the diagnostic criteria for NTM pulmonary disease were fulfilled.1
M. xenopi is a ubiquitous, thermophilic, slow-growing NTM. This organism is found in freshwater and has been isolated from water samples collected in homes and hospitals.1 M. xenopi appears to have a variable geographic distribution. It has been recovered frequently from clinical specimens in the United Kingdom, northwestern Europe, and Canada; rarely has it been isolated in the U. S. prior to the AIDS epidemic.11 M. xenopi is a very rare pathogen of pulmonary disease in Asian countries, including Japan and Korea. Recently, we reported the clinical significance of NTM isolates from respiratory specimens in Korea.4 In that study, only one of more than 1,500 isolates of NTM from about 800 patients was confirmed to be M. xenopi, and its clinical significance was doubtful.
However, M. xenopi is increasingly recognized as a cause of pulmonary infection. Clinical illness typically presents as an indolent, cavitary lung infection in middle-aged men. Most of those patients have a history of underlying chronic pulmonary disease.1 Conditions predisposing an individual to M. xenopi infection include previously treated pulmonary tuberculosis, chronic obstructive pulmonary disease, diabetes mellitus, alcoholism, and a bad postoperative state.5-7,12,13 The classic radiographic appearance of M. xenopi pulmonary disease is a cavitary, apical pulmonary process.5-7,12-14
The optimal therapy and duration of treatment for pulmonary disease secondary to M. xenopi has not been established. Current protocols for M. xenopi infection recommend chemotherapeutic combination with three or four drugs and an overall treatment duration of 18-24 months.1,7,15 The in vitro susceptibility to anti-tuberculosis agents is variable, although enhanced drug activity has been demonstrated with the combination of rifampicin and streptomycin, or rifampicin and ethambutol.16 There was no correlation between treatment outcome and in vitro susceptibility.5 The cornerstone of treatment for M. xenopi infection is currently a combination of rifampicin and ethambutol. Although about 70% of clinical isolates of M. xenopi are resistant to ethambutol, ethambutol is strongly recommended.5 A prospective, randomized study found that the addition of isoniazid is of little or no value in the treatment of M. xenopi infection.5 Some studies of clarithromycin-containing regimens demonstrated good bactericidal activity.17,18 In addition, the successful treatment of M. xenopi infection with a combination of clarithromycin and newer quinolones has also been described.19
The death rate of pulmonary disease secondary to M. xenopi is as high as 70% within five years of onset.5 Although underlying comorbidities might be a major factor determining the death rate, the poor response to antibiotic treatment is alarming. Given the relative ineffectiveness of medical therapy, surgery is an important alternative in patient who can tolerate it.20 Although some investigators have reported success with surgical therapy, others have had disappointing results.6,13
Based on recommended treatment regimens and the results of in vitro susceptibility testing, we initially selected a combination of clarithromycin, rifampicin, ethambutol, and streptomycin for our patient. After four months of antibiotic therapy, moxifloxacin was added due to adverse effects with streptomycin and disease progression. Finally, pulmonary resection was performed. Unfortunately, the patient expired because a bronchopleural fistula developed and led to pneumonia and respiratory failure.
In conclusion, Mycobacterium xenopi is considered to be a cause of pulmonary infection in immunocompetent patients with pre-existing lung disease. This case serves as a reminder to clinicians that the incidence of NTM infection is increasing in Korea, and that unusual NTM organisms are capable of causing disease in non-immunocompromised patients.

 XML Download
XML Download