

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Minimally invasive options in urologic surgery are increasing. The addition of the da Vinci™ robot system (Intuitive Surgical, Inc., Mountain View, CA, USA) to urology has brought about new, exciting, alternative approaches. Currently, the radical prostatectomy is considered the gold standard in the management of localized prostate cancer.1 Over the last 10 years, laparoscopic radical prostatectomy (LRP) has developed as a less-invasive alternative to the conventional open radical prostatectomy.2-4 Advantages of LRP include reducing the length of hospitalization, the degree of postoperative disability, and the duration of convalescence. Overall success rates have been equivalent to those reported with open prostatectomy.5,6 In our institution, LRP has been performed in eight cases, and excellent outcomes were achieved in those patients. However, LRP has limitations: a steep learning curve, difficult to undertake without advanced laparoscopic experience, counterintuitive movements, rigid instruments, two-dimensional images, and less-than-optimal ergonomics.7
In recent years, robot-assisted LRP (rLRP) has emerged as a feasible treatment option for patients with organ-confined prostate cancer to overcome LRP limitations. An rLRP performed with the da Vinci™ surgical system represents the latest minimally invasive technique for the treatment of prostate cancer. The instruments have a total of seven degrees of motion (six degrees of freedom and grip), EndoWrist instrumentation, high resolution 3D vision, intuitive motion, and filtration of unwanted physiologic tremors. The da Vinci™ robot system has several features in performing rLRP: 1) superior visualization of tissue planes and the neurovascular bundles, 2) meticulous dissection of the prostate and surrounding structures, and 3) precise suturing of the urethrovesical anastomosis.
Recently, we performed the first four cases of rLRP in the Republic of Korea. This is our report on the techniques and experiences of rLRP.
CASE REPORT
Between July 2005 and October 2005, we performed rLRPs in a total of four patients with localized prostate cancer. The mean age was 60.8 (range: 45-70) years old, and the mean PSA value was 5.8 (range: 1.37 to 9.8) ng/mL. The Gleason score ranged from 4 to 7 and the clinical stage of the four cases was T1c (Table 1). After staging, which included pelvic magnetic resonance imaging (MRI), the decision to perform an rLRP was made. The first patient had a past history of two transurethral resections of the prostate. The fourth patient had undergone neoadjuvant hormonal therapy by the primary physician. There was difficulty in performing rLRP on these two patients, in that bladder neck dissections and vas deference and seminal vesicles dissections.
The procedure was performed with the patient under general anesthesia in a modified lithotomy position. The patient was also carefully secured to the operating table after confirming that all pressure points were well padded. The table was set in a steep Trendelenburg position and fully lowered. A standard skin preparation was performed from the xiphoid process to the pubic symphysis and genitalia. An 18 Fr. Foley catheter was inserted into the bladder. An orogastric tube was also placed.
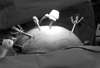
After the establishment of pneumoperitoneum with a Veress needle, six ports were placed (Fig. 1). The robotic camera arm was inserted through a 12-mm optical trocar at the supraumbilicus. The working arms of the robot were placed pararectally below the level of the umbilicus through 8-mm robotic ports (Intuitive Surgical). The first assistant surgeon controlled the traditional laparoscopic instruments through an additional 12-mm port. A suction cannula with a 5-mm port was placed ipsilateral to the assistant's side between the camera and the robotic port. The second assistant surgeon controlled the laparoscopic instruments through a 5-mm port placed at the opposite site of the first assistant's 12-mm port.
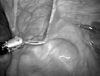
After the placement of the 12-mm camera port, a peritoneoscopy was carried out with a 00 laparoscope (Fig. 2). The bladder dissection started with an incision by a monopolar spatula electrode. The incision was lateral to the medial umbilical ligament. The incision extended inferiorly to the vas and superiorly to the anterior abdominal wall. When the dissection was performed downward, the glistering arch of the pubic bone (laterally) and the edge of the bladder (medially) were seen. The fat that was underneath the pubic symphysis, over the apex of the prostate, lateral from the endopelvic fascia, and near the prostatovesical junction, was swept away, fulgurated, and excised. Once the puboprostatic ligaments were cleared and the superficial dorsal vein was made visible, the superficial dorsal vein over the prostate was coagulated and transected.
The endopelvic fascia was incised on its line of reflection from the levator ani muscles arching laterally. This was done to enter the plane separating the prostate from the levator ani muscles. This process was accomplished with blunt dissection by a monopolar spatula electrode. This dissection was extended proximally to delineate the junction between the prostate and the bladder. The dorsal vein complex and the apex of the urethra were freed laterally by separating the collar of the puboperinealis muscles. The prostate apex was freed as much as possible. The deep dorsal vein was ligated with an EndoGIA stapler in the first two cases. However, in the last two cases, the deep dorsal vein was not ligated and the prostatic fascia was preserved (No touch technique).8,9 The endopelvic fascia was not excised, and only the prostatic fat tissue was dissected and removed.
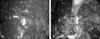
To identify the bladder neck, a Foley ballooning was drawn out. At the anterior surface, fat, fibrous tissue, and converging detrusor muscle fibers were divided to enter the bladder neck. The incision of the anterior bladder neck exposed the Foley catheter balloon, which was deflated (Fig. 3A). The catheter was pulled up to delineate the rest of the bladder neck. The bladder neck was further incised with tailoring according to the presence of medial, lateral, or intravesical projecting lobes of the prostate. The posterior bladder neck was also divided carefully to avoid injury to the urethral orifice (Fig. 3B). With the aid of visual cues, meticulous posterior dissection was performed to expose the anterior layer of the Denonvillier's fascia. The transverse incision in the fascia revealed the vas deferens and the seminal vesicles. After the dissection of the vas and seminal vesicles surroundings, the vas and seminal vesicles were lifted up. The anterior traction on these structures exposed the prostatic pedicles.
The incision of Denonvillier's fascia and dissection posterior to the apex of the prostate were performed. The prostatic pedicles were controlled by clipping or cauterizing with bipolar Maryland forceps. During this preservation of the neurovascular bundle, the lateral periprostatic fascia was preserved. The resulting veil of tissue is known as the Veil of Aphrodite. The apical dissection and transection of the urethra was performed. Periapical biopsies were obtained for frozen-section examination. If the dissected bladder neck was wide, the posterior bladder neck was reconstructed by 3-0 monocryl suturing.
A 300 telescope was used during the creation of the anastomosis. A single suture was prepared by tying the tails of two 3-0 monocryl sutures on a UR6 needle. A running anastomosis was created using the previously described suturing technique (Fig. 4. A and B).10 An 18 Fr. silastic Foley catheter was introduced, and the balloon was inflated to 10cc. A final urethrovesical anastomosis suture was then performed. The bladder was filled with 150mL of saline with the balloon of the catheter away from the bladder neck to test the patency and leakage of the anastomosis.
A Hemovac was placed through a 5-mm port in the extraperitoneal space. The specimen entrapped in the bag was removed by enlarging the port site incision at the umbilicus. Subsequently, all port sites were closed appropriately.
Table 2 shows the patient clinical outcomes. In four cases, the mean operative time was 392.5 minutes, which was longer than that required for the LRP (8 cases: 302.1 minutes). The duration appears to have been reduced by an increase in the surgeon's experience (learning curve). The mean estimated blood loss was 312.5mL. There were no major intraoperative or postoperative complications. A clear liquid diet was started on postoperative day 2. The mean postoperative hospitalization was 8 days. Although the first two patients could have been discharged on day 3, the discharge was delayed to 11 days. The delay was caused by minor complications including left buttock area pain. This was thought to be due to an ischemic injury caused by a long operating time. The last two patients were discharged on postoperative day 5. The bladder catheter was removed after 14-21 days. The pathological examinations are summarized in Table 2 and showed negative surgical margins.
DISCUSSION
The gold standard treatment of localized prostate cancer, radical retropubic prostatectomy (RRP), has evolved over the last three decades. It has become a precise, sophisticated procedure with minimal mortality and excellent surgical outcomes. To match this operation by minimally invasive means, minimal morbidity, and excellent functional and oncologic outcomes is an arduous task. After the first application of laparoscopic surgery to prostate cancer management in 1992, robot-assisted laparoscopic radical prostatectomy was first performed in 2001. Since then, its use has proved to be successful.
The da Vinci™ robot appears to be advantageous in providing better visibility and allowing the operating surgeon to maneuver the tips of the instruments with greater degrees of freedom than its counterpart-manual laparoscopy. The main advantage of robot-assisted laparoscopic surgery appears in radical prostatectomy, especially during the preservation of the neurovascular bundle. It also has been shown that intracorporeal suturing can be learned faster with the robot than with manual laparoscopy in controlled laboratory studies.11 Currently, the applications of robot-assisted laparoscopic surgery in urology are quickly expanding.
Large series reports of robot-assisted radical prostatectomy by various authors have presented the development of the structured program, in comparison with open and laparoscopic surgery, nuances of techniques, and outcome analysis of functional results with follow-up popularized the procedure12-15 and have led to a change in the perception of robot-assisted radical prostatectomy for the management of localized cancer of the prostate. In reports from worldwide centers, there has been no noticeable difference in terms of oncologic completeness and the margin-positive.
Robotic prostatectomy has also been associated with shorter overall operative times, shorter anastomotic times with a better anastomosis, and improved preservation of the neurovascular bundles. All of these results translate to earlier continence and return of erectile function for most patients.16,17 While all the aforementioned approaches have been shown to be feasible, we believe that the da Vinci™ robot helped us in performing the anastomosis with greater ease. Furthermore, the surgical dissection of the different planes which was necessary to identify the structured prostate-vesical junction (Denonvillier's fascia et al.) was facilitated by the three-dimentional surgical field at the console. Despite the lack of tactile feedback with the da Vinci™ robotic system, dissection and anastomosis were readily performed without any complications. The role of the assistant surgeon in facilitating tactile feedback when needed is critical. The assistant surgeon can use instruments to identify different landmarks and help guide the operating surgeon behind the console.
We performed the bilateral nerve sparing without pelvic lymphadenectomy. All steps in the operation were completed with the da Vinci™ robotic system. The system placed instrument movements under direct, real-time control. It also provided great dexterity and precision. Hand tremor was eliminated by the system. The master range of motion allowed full, natural movements that were transmitted accurately to the surgical arms.
Our four cases of robot-assisted laparoscopic radical prostatectomy concluded that the surgery can be performed safely. The results of the present robotically assisted surgeries in regard to local cancer control, hospitalization, and postoperative course were similar to those of standard laparoscopic radical prostatectomy.
Although the present report only records our initial and limited experience, we confirmed that rLRP can be performed satisfactorily using the da Vinci™ system. An rLRP is a safe and feasible approach. It will become one of the standard options for the management of localized prostate cancer.



 XML Download
XML Download