

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Chronic expanding hematoma of the thorax is a rare disease entity and usually presents as a slowly expanding mass in patients with histories of either thoracoplasty or tuberculous pleurisy.1,2 As with all chronic expanding hematomas, symptoms may arise months or years after trauma or surgery and most cases of growing hematomas have been detected in patients with no history of hemophilia or any other hemorrhagic diatheses. The treatment of choice in these cases is surgical resection because it is quite difficult to distinguish these masses from other malignant tumors, which appear in combination with chronic empyema, including malignant lymphoma, soft tissue sarcoma and squamous cell carcinoma.3-5
In this report we describe a case of chronic expanding thoracic hematoma that developed into a very large mass over a long period of time.
CASE REPORT
A 67-year-old woman was admitted to our hospital complaining of increasing dyspnea. Thirty-seven years earlier, at the age of 30, the patient had undergone a right pneumonectomy for the treatment of pulmonary tuberculosis and has since pursued a normal active life, until 6 months prior to her admission for increasing shortness of breath. The patient had no history of hemophilia or any other hemorrhagic diatheses. Upon admission, the patient exhibited anemia, with a hemoglobin level of 7.9g/dL, but her other lab findings were normal.
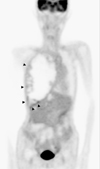
The chest radiograph obtained at admission, revealed an opacified right hemithorax with tracheal deviation and a shift of the midline mediastinal structures to the left (Fig. 1), which had progressed as compared with images taken 1 year prior. Chest computed tomography (CT) revealed a huge mass with central low attenuation and a thick wall containing flecks of calcification replacing the entire right hemithorax (Fig. 2). The lung window images revealed no abnormal findings in the left hemithorax. Positron emission tomography with fluorodeoxyglucose (FDG-PET) images revealed a huge mass replacing the entire right hemithorax with central photon defects and mildly increased FDG uptake in the anterior lower portion (maximum standardized uptake value = 3.7) (Fig. 3). We then conducted a fluoroscope-guided percutaneous lung biopsy. The biopsy specimens revealed necrotic tissue only, with an absence of viable cells.
The tumor was extirpated under a clinical diagnosis of chronic empyema combined with a malignancy such as malignant lymphoma or soft tissue sarcoma. A large amount of dark, reddish-brown fluid and large material with a solid fibrinous consistency, encompassed by a dense fibrinous capsule, was curetted and removed. The pathological findings of the pleura included dense fibrocollagenous tissue with dystrophic calcifications and focal necrosis. Samples sent for histopathological and microbiological analysis revealed no evidence of neoplasia or infection. The patient's postoperative course was uneventful and the patient was discharged without complications.
DISCUSSION
Chronic expanding thoracic hematoma is a rare disease entity. Affected patients typically have histories of medical or surgical therapy for the treatment of tuberculosis. The majority of reports of chronic expanding hematoma of the thorax have come from Japan.1,2,6-8 Recent literature from the United States also suggests a certain incidence of chronic expanding thoracic hematoma in Western countries.9,10 However, to the best of our knowledge, no such cases have been reported in Korea until now.
Other than the rare entity which originates in the thorax, chronic expanding hematomas can occur in a variety of locations.11 Although most hematomas resolve spontaneously, a few can persist for long periods, forming slowly expanding space-occupying masses. Subdural hematomas are the most widely reported example of expanding hamatomas.11 The pathogenesis of chronic expanding hematomas has yet to be elucidated in any detail. Labadie and Glover12 have theorized that this self-perpetuating expanding process is attributable to the irritant effects of blood and the products of its breakdown, which induce repeated episodes of bleeding from the capillaries in the granulation tissue. Clinically, intermittent episodes of bleeding, probably due to respiratory motion and coughing, may be responsible for progressive increases in the volume of these hematomas. As was seen in our case, in which old blood and necrotic debris without bacteria, including mycobacteria, were detected in the patient's intrapleural lesion, chronic expanding hematomas of the thorax tend to be nonpurulent and usually display no evidence of bacterial infection.1
The most frequent presenting symptom in such cases is dyspnea, usually related to lung compression, or a slowly growing mass in the chest wall, both of which normally develop 30 years or more after treatment for tuberculosis. Radiologically, chronic expanding thoracic hematomas tend to appear as intrathoracic masses. CT findings usually reveal a heterogeneous mass with a wall of variable thickness, which often harbors peripheral regions of calcification.1,10
Surgical resection at an early stage is the treatment of choice in such cases to prevent mediastinal deviation and extrathoracic protrusion. Surgery is also warranted because it is difficult to differentiate this condition from malignancies, such as malignant lymphoma, soft tissue sarcoma, or squamous cell carcinoma.3-5 The surgical procedure conducted should be a complete resection even if the tumor is benign, because incomplete treatment, such as drainage and curettage of the contents, may result in massive bleeding from the hypervascular subcapsular lesion.1
FDG-PET images of chronic expanding hematoma are not widely available. In one case report of a patient with chronic expanding hematoma in the pelvis, an increased FDG uptake in the peripheral rim of the mass was noted and the maximum standardized uptake value was 3.10, suggesting a hematoma associated with a malignant lesion.13 In our patient, FDG-PET images of the lesion revealed central photon defects with focally increased FDG uptake in the anterior lower portion and the presence of a malignant lesion could not be excluded from these findings.
In conclusion, chronic expanding hematoma of the thorax is a very rare condition, but should be considered in the differential diagnosis in cases in which an expanding mass is observed in the thoracic cavity, especially when the patient has a history of tuberculous pleurisy, thoracotomy, or thoracic trauma.


 XML Download
XML Download