

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
In removing orbital foreign bodies, accurate localization of the foreign body in the orbit and the choice of a safe and appropriate surgical procedure are vital.1 Lateral orbitotomy, one possible surgical procedure, does not afford a good view of the retrobulbar foreign body2 and might apply excessive pressure to the doubly perforated eyeball when we look for the retrobulbar foreign body. Therefore, we consider the transcranial approach to be useful for removing a retrobulbar foreign body that is difficult to approach.
CASE REPORT
A 63-year-old man presented with a penetrating injury to his left eye that had occurred that day while he was working with industrial machinery. Slit lamp examination revealed a corneoscleral laceration (9 mm), hyphema, a traumatic cataract, and vitreous hemorrhage in the left eye. Computed tomography of the orbit demonstrated a foreign body (likely a piece of iron) which had passed through the left eyeball and was located in the posterior orbit (Fig. 1A). Visual acuity (VA) in the left eye was limited to the perception of hand motion. Nevertheless, the patient had no trouble distinguishing shades of red, green, and blue.
On the day of admission, corneoscleral suturing, phacoemulsification of the cataract, and vitrectomy with posterior vitreous detachment were performed. After the vitrectomy and clearing of the vitreous cavity with a backflush needle, we observed a penetrating wound in the fundus, but did not see any of the object. The eyeball was so hypotonic that we could not apply endolaser photocoagulation around the penetrating wound and had to perform a fluid-gas exchange with 20% SF6 gas. We had to leave the second penetrating wound unsutured. Postoperatively, the patient was treated with intravenous ciprofloxacin (400 mg/day) and tobramycin (160 mg/day). Drops of 0.3% ciprofloxacin and 1% prednisolone were given every 4 hours for 2 weeks. The day after the surgery, slit lamp examination showed no leakage around the corneoscleral laceration, and there was a fibrinous pupillary membrane. A color perception examination was normal, and the intra-ocular pressure (IOP) in the left eye was 13 mmHg. On postoperative day 14, we could not see the retina because of the vitreous hemorrhage. The IOP was 8 mmHg. Light projection and color perception were normal.
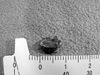
On postoperative day 15, frontal craniotomy and superior orbitotomy were performed to remove the foreign body (8 × 7 mm in size) (Fig. 2). After placing the patient in the supine position, a bicoronal scalp incision was made just anterior to the tragus of the ear on the left side and extended approximately to the superior temporal line on the right side. Subperiosteal dissection was used to elevate the entire frontal flap and the temporalis muscle. The supraorbital nerve was identified and freed with a small osteotome. A rectangular shaped frontal bone flap with one burr hole was then made using a high-speed air drill. Then, the subperiosteal dissection was extended into the orbit so that the periorbital tissue was displaced from the superior orbital roof. A frontal bar osteotomy was done with a high-speed drill, and the anterior orbital roof was fractured forward. After extradural dissection to the region of the optic canal, the remaining orbital roof was removed with a rongeur. Under an operating microscope, the periorbita was incised after identification of the frontalis nerve and the levator palpebrae muscle. The periorbital fat was isolated, and dissection was carried down bluntly through the medial side of the levator palpebrae with the aid of intraoperative ultrasound and self-retaining retractors. Meticulous hemostasis was performed with bipolar forceps during the procedure. The foreign body was identified just deep to the optic nerve between the medial and inferior rectus muscles and was removed using basket retrieval forceps. There were some inflammatory changes (dark yellow discoloration) around the foreign body. Irrigation was done with saline mixed with antibiotics. After suture of the periorbita, orbital roof was reconstructed using 24 G-wire fixation with the inner table of the frontal bone flap. The frontal bar was realigned with 2 microplates. After placement of the frontal bone flap with a bone fixator, the scalp wound was closed in layers.
On the first day after the second operation, VA in the left eye consisted of light perception only. Orbital edema slightly limited globe movement. The vitreous hemorrhage was categorized as Grade IV. Ten days after the second operation, the corrected VA in the left eye was 20/100, and the degree of vitreous hemorrhage had reduced to Grade I to II. After 6 months, the corrected VA had improved to 20/30, and the vitreous hemorrhage had cleared completely. A white fibrous lesion was still seen at the site of the penetrating wound inferior to the optic disc (Fig. 3).
DISCUSSION
The removal of a foreign orbital body is complicated. Posterior foreign bodies have an increased risk of motility disturbance and optic neuropathy after surgical removal.3 Some studies on rabbits report significant iron accumulation in ocular tissues after ocular penetration with iron,4,5 while others report that metallic foreign bodies can be retained safely in the majority of cases.3,6 In our case, the foreign body was an iron-containing particle. Based on the risk of an iron foreign body and its close proximity to the sclera, we decided to remove the intra-orbital foreign body after discussing the potential sequelae of a retained iron foreign body with the patient. After removing the foreign body, we confirmed its metallic nature using a magnet. There were no signs of iron accumulation in the patient's eye.
In this case, the transcranial approach was considered the most appropriate for removing the retrobulbar foreign body, as it provides wider exposure of the orbital cavity and results in fewer surgical complications and less orbital tissue damage than lateral orbitotomy.2,7-9
Our patient had a double-perforation injury of the eyeball and we were unable to suture the posterior wound. Therefore, applying excessive pressure to the eyeball immediately after the first operation could have increased the risk of leakage from the posterior, unsutured eyeball wound. We minimized pressure on the eyeball using a transcranial approach, and the foreign body was successfully removed by a neurosurgeon. Although we could not suture the posterior wound, it sealed itself and there were no complications to the retina. We think that complete vitrectomy with posterior vitreous detachment at the correct time performed by a retina specialist and with minimal pressure on the eyeball while removing the foreign body by use of a transcranial approach contributed to the positive results.
When it is necessary to remove orbital foreign bodies that are not readily removable because of their location, a transcranial approach is most likely to minimize complications, although the approach calls for technical competence and is time-consuming.


 XML Download
XML Download