

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Refractures are fractures occurring at the initial fracture site. These fractures make up about 1 in 1000 of all children's fractures, and are known to frequently occur in the forearm.1-4 Although adult refractures have been frequently studied in the past,5,6 there are only a few studies involving children. Difficulty in controlling external factors confounds statistical analysis. Known risk factors include disturbance of the local blood flow,1 repeated forces exerted on the same area,7 inappropriate reduction,8 incomplete bony union,9,10 early cast removal,11 greenstick fractures,8 inappropriate technique of cast immobilization, malunion, and disuse osteopenia.12
Refractures can be classified into early and late forms. Early refractures occur through the immature callus and occur due to a short period of immobilization. Late refractures, however, occur in the remodeled bone and are related to the patients' activity.8 In this study, we evaluated the clinical and radiological characteristics of upper extremity refractures in children. The goal of this study was to determine the frequently occurring fracture area, fracture mechanisms, and fracture risk factors.
MATERIALS AND METHODS
We performed a retrospective study using the medical records (dated from January 1997 to December 2003) from our institution. During this period, 32 patients (aged less than 15 years old), were diagnosed and treated for refractures in the upper extremities. Refractures involving the hands and wrists were excluded. Patients with systemic diseases such as osteogenesis imperfecta and cerebral palsy, or those with different fracture site from the initial one, were also excluded. The remaining 18 cases used in this study consisted of 13 boys and 5 girls. Eight cases involved the right upper extremity and ten cases involved the left. The study subjects were divided into three groups according to the initial fracture site: Nine cases were classified and included in the supracondylar fracture group, three cases as the lateral condyle fracture group, and six cases as the forearm bone fracture group. We investigated several parameters, including the time interval from the initial fracture to the refracture, refracture mechanism, and the treatments of both the initial and refracture were investigated. The existence of angulation or malrotation before the refractures was noted using the plain radiographs of the initial, primary fracture, postoperative radiographs, as well as those taken during the follow-up period. In the supracondylar fracture group, the initial fractures in six cases were treated with cast immobilization, and three with closed reduction and percutaneous pinning. One lateral condyle fracture was treated with closed reduction and percutaneous pinning, and two were treated with open reduction and percutaneous pinning. In the forearm bone fracture group, five patients had fractures at both the radius and ulna, and one had an ulnar fracture only. Five of those cases were treated with simple cast immobilization, and one was treated with internal fixation using an intramedullary nail.
RESULTS
Age of initial fracture and time interval from initial fracture to refracture
Initial fractures occurred at the average age of 3 years and 8 months (range, 13 months-12 years), and refractures at the average age of 5 years and 5 months (range, 3 years-12 years and 3 months). Initial supracondylar fractures occurred at the average age of 3 years and 4 months (range, 13 months-5 years and 4 months), and refractures at the average age of 5 years and 1 month (range, 3 years-8 years and 1 month). Lateral condyle fractures occurred initially at the average age of 2 years and 10 months (range, 2 years and 1 month-3 years and 9 months), and refractures at the average age of 5 years and 11 months (range, 4 years and 8 months-7 years). Initial forearm bone fractures occurred at the average age of 5 years and 9 months (range, 3 years and 4 months-11 years and 11 months) and refractures at the average age of 6 years and 8 months (range, 4 years and 5 months to 12 years and 3 months).
The occurrence of refractures in all children varied from 1.8 months to 59 months after the initial fracture. However, there were differences in the peak age of occurrence, depending on the initial fracture sites. In the supracondylar fracture group, refractures occurred at the average of 26 months after the initial fracture. With the exception of one case, all fractures were late refractures that occurred after a complete union and bony remodeling. Refractures in the lateral condyle fracture group occurred at the average of 37 months after the initial fracture, and they were classified as late refractures. On the other hand, in the forearm bone fracture group, all the refractures occurred within 5 months of the initial fracture and were classified as the early type with incomplete bony remodeling.
Anatomical sites of refractures and their mechanisms of injury
In the supracondylar fracture group, two refractures were supracondylar region, and seven involved the lateral condyle. In the lateral condyle fracture group, one case involved the supracondylar region and two involved the lateral condyle. Out of the nine refractures occurring at the lateral condyle, seven were complicated with cubitus varus prior to the refracture. In the forearm bone fracture group, all the refractures occurred at the same sites as the initial fractures. Five cases were treated with the application of a cast, and one was fixed with intramedullary nail. Indirect forces, such as an out-stretched hand and elbow injury, were the most common mechanisms responsible for both the initial and refractures.
Underlying angulation deformity before refracture
Among the twelve refractures occurring at the distal parts of the humerus (i.e. the supracondylar region and lateral condyle), seven were complicated with cubitus varus prior to the refractures. The average carrying angle was -11.1 degrees, and had a Baumann's angle of 15.9 degrees. Six cases of cubitus varus were due to malunion of the initial supracondylar fracture, and one was due to overgrowth at the lateral condyle fracture site. On the other hand, five cases were uncomplicated by cubitus varus: one case involved an early refracture, occurring within eight weeks of the first fracture, and one case was a repeat fracture secondary to direct injury by a stick.
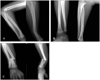
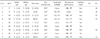
Four of the six forearm bone fractures were initially greenstick fractures, and they were angulated anteriorly. The anterior angulation of the fracture site was not properly corrected, and it was observed that there was not a complete bony union on the convex side of the refracture. Five of the six repeat fractures were complete fractures of both the radius and ulna, and one was a complete fracture of the ulna only. The average cast immobilization period was 8.5 weeks (range, 4-20 weeks), and there were four cases of early cast removal, occurring 9 weeks after the initial fracture (Fig. 1, 2, 3, Table 1, 2, 3).
DISCUSSION
We observed the time interval between the initial fracture and the refracture and analyzed the responsible anatomical factors. We found that these parameters differed based on the initial fracture sites. The time interval before the refractures of the distal portion of the humerus was longer than those of forearm bone refractures. This is probably due to faster bony union in the distal part of the humerus, aided by sufficient blood flow to the fracture site. In refractures involving the distal part of the humerus, many had already been complicated by cubitus varus, and the lateral condyle fracture was the most common form. According to Davids,12 the lateral side of the elbow joint connecting the radius, capitellum, and humerus would have varus alignment when the subject falls with the arm out-stretched. Torsional and shearing forces converge on the lateral side of elbow joint-a site that is already malaligned with a varus deformity-which is a predisposing factor for fracture. In this study, refractures of the supracondylar region occurred less often.
Takahara13 commented that the metaphysis is thickened after a supracondylar fracture, and that this thickening protects the fracture site from the external forces. In contrast, the epiphysis, or growth plate, weakens against the fracture. If cubitus varus occurs, operative correction should be considered. We believe that it is important to prevent malunion such as cubitus varus in fractures involving the distal parts of the humerus. Also, patients with cubitus varus need to be warned of higher possibility of secondary fractures, and must be advised to refrain from extreme contact activities. On the other hand, most refractures occurring in the forearm were classified as early type. Refractures occurred at areas of incomplete bony union within 5 months of the primary fracture. The so-called "greenstick fracture" has been known to be susceptible to refractures.8,10,14 Bony union on the convex side of the fracture that has a loss of cortex continuity is delayed due to the elasticity of the concave side, which maintains continuity of the cortex. Fillipe10 notes that the angulation from inadequate reduction of the forearm bone fracture may delay bony union. To our knowledge, there are no studies regarding complete anatomic reduction without angulation, and its role in refractures. Since bony union is slower in the diaphysis than in the metaphysis, we believe that anatomical reduction of a forearm diaphyseal fracture is crucial in order to prevent a refracture, as well as preserve function. In cases involving a greenstick forearm fracture, we recommend breaking the cortex of the non-fractured side in order to have complete reduction and to eventually prevent a refracture. It is also better to remove the cast when the bony union has been verified, as the diaphysis is more likely to experience tensional forces than the metaphysis.
In evaluating the factors involved in a refracture, we did not consider the patients' habitual behaviors or seasonal variations. However, considering that 13 of 18 cases were boys, and that boys are relatively more active than girls in sports, the patients' compliance would be another factor affecting reoccurrence. Our retrospective study showed that in cases where cubitus varus occurred after the fracture of the distal humerus, a secondary fracture is more likely, even after complete bony union and remodeling. In the cases of forearm bone fractures, the existence of a greenstick fracture, incomplete bony union, and residual angulation were the major risk factors for a secondary fracture. We believe that one should take into account the risk factors and the site of the primary fracture in order to prevent a refracture in each bone. Further prospective studies regarding the relationship among each factor should be followed.




 XML Download
XML Download