

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Most ECCs are polypoid type, which undergo the adenoma to carcinoma sequence. However, it must be emphasized that non-polypoid lesions also occur.1 These are classified as protruded, slightly elevated (small flat adenoma), lateral spreading tumor (LST), and depressed type.2 The existence of flat or depressed type ECC has been reported in Japan, and may have higher malignant potential than polypoid type ECC.3
In this report, we present the case of a 65-year-old female diagnosed with a small sized and histologically well-differentiated lesion of depressed type ECC, however, with extensive lymph node metastasis and no regional lymph node involvement.
CASE REPORT
A 65-year-old female with a significant medical history for hypertension and diabetes mellitus type II, presented with a 2-month history of low abdominal discomfort, bowel habit changes, and weight loss. Physical examination revealed no abnormal findings, except for slight lower abdominal tenderness. Abnormal laboratory studies included an elevated serum CEA level of 7.65ng/ml, but CA19-9, CA125 was within normal range.
Evaluation included colonoscopy, which disclosed a 1.0cm sized depressed mucosal lesion with marginal elevation on the proximal transverse colon (Fig. 1). Absence of air deformation was present, signifying a more invasive cancer. Histologic evaluation of biopsied tissue showed adenocarcinoma. Because depressed type ECC has a high incidence of deep submucosal invasion, we recommended surgical removal of this tumor.
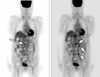
Staging workup included abdominal CT (computed tomography) scan (Fig. 2), which illustrated questionable wall thickening in the proximal transverse colon and multiple lymph node enlargements along the root mesentery, aortocaval, left paraaortic, and left common iliac lymph node axis. This suggested extensive lymph node metastasis; however, there was no regional lymph node enlargement in the transverse colon paracolic area. EGD (esophagogastroduodenoscopy) to rule out other origin of the tumor revealed no abnormal findings. PET (positron emission tomography) scan (Fig. 3) demonstrated multiple lymph node metastases to the left supraclavicular fossa as well as left paraaortic and aortocaval lymph node enlargement.
We performed a right hemicolectomy for the purpose of accurate diagnosis and treatment by resection of primary colon mass and metastasized lymph nodes, if possible.
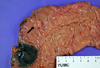
Findings included a 1 × 1cm sized mass on the proximal transverse colon with grossly enlarged paraaortic, middle colic, ileocolic lymph nodes without regional lymph node enlargement and ascites (Fig. 4).
Histologic evaluation showed well-differentiated adenocarcinoma extending to the deep submucosa with frequent lymphovascular permeation and no regional lymph node involvement of 21 resected lymph nodes (Fig. 5).
The patient was treated with several chemotherapeutic regimens; however, the disease progressed to carcinomatosis, and she decided to continue with supportive care only without further chemotherapy.
DISCUSSION
Early colorectal carcinoma is defined as "invasive carcinoma that has not spread in the direction continuity beyond the submucosal layer, regardless of the presence of blood-borne or lymphatic metastasis for the TNM classification, these lesions are T1NxMx".4
A classification for T1 lesions has been developed in Japan,5,6 this classification is essentially for a sessile lesion in which the submucosal invasion is divided into sm1 (invasion in upper one-third), sm2 (invasion in the middle one-third), and sm3 (invasion in the lower one-third).2
ECC seems to have two patterns of progression. The first is a relatively slow development of cancer in an adenoma; this is demonstrated by a polypoid growth eventually becoming cancerous. The second is a more controversial rapid and deep cancerous invasion; this is demonstrated by non-polypoid growth arising de novo and not found to be associated with adenoma.7 These non-polypoid colorectal neoplasm are grossly classified into three groups: slightly elevated (small flat adenoma), laterally spreading (LST), and depressed.2
Kariya et al. first described depressed type ECC in 1977.8 These tend to be invasive even when small sized,9 and are more malignant than flat adenomas.
The incidence of submucosal cancer is higher in ECC with depression (IIc, IIc+IIa, and IIa+IIc) than without depression or in the elevated type (Ip, Isp, and Is).10 In one study, rate of submucosal invasion was 2.1%, 0.05%, 8.2%, and 29.5% for polypoid, small flat adenoma, LST, and depressed lesions, respectively.2
Therefore, depressed lesions should always be treated. Endoscopic mucosal resection (EMR) technique can be used to remove lesions confined to the mucosa or that only slightly invade the submucosa. Additional surgical resection would be required for resected specimens demonstrating massive submucosal invasion or vessel permeation on histologic analysis; otherwise, risk of recurrence or metastasis would be high.2
The incidence of lymph node metastasis in submucosal invasive cancers has been reported to be less than 15%, with only 0 to 3.2% of cases having carcinomas with shallow invasion of the submucosa (sm1 carcinomas).7,11 Many investigators have demonstrated that lymph node metastasis is closely associated with depth of submucosal invasion, growth patterns (polypoid or non-polypoid), lymphovascular invasion, and histologic subclassification at the deepest invasive portion.7,11-13 Generally, poorly differentiated carcinomas have a high risk of lymph node as well as distant metastasis.14
Distant metastasis to the liver and lung had been reported in early invasive colorectal cancer, but all had been associated with primary tumor in the rectum, a sessile type configuration, sm3 level of invasion, and positive lymphatic invasion.7
In the case presented, the lesion was an ECC of small and depressed type, for which detection is difficult and incidence of submucosal invasion is high. The risk factors for metastasis included depressed type, submucosal invasion (sm3, submucosal invasion in the lower one-third), and lymphovascular permeation. The surprising fact in this case was that metastasis was very extensive compared to T staging, including a high level of lymph node involvement such as the aortocaval and paraaortic nodes without regional lymph node involvement, and that it presented well-differentiated histology.
In conclusion, we recommend careful colonoscopic examination to detect small and flat depressed lesions, and even if the lesion is small or flat, the possibility of distant metastasis should be considered.



 XML Download
XML Download