

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Primary neoplasms of the heart are rare. Autopsy series report a combined incidence of 0.0017% to 0.28% for both benign and malignant primary cardiac tumors.1,2 Malignant tumors, the majority of which are sarcomas, comprise up to 25% of cardiac neoplasms.3 Undifferentiated cardiac sarcomas primarily develop on the left side of the heart and cause signs and symptoms related to pulmonary congestion, mitral stenosis, and pulmonary vein obstruction.4
We present a case of cardiac undifferentiated pleomorphic sarcoma that presented as acute pulmonary edema, and was preoperatively diagnosed as a benign myxoma of the left atrium.
CASE REPORT
A 37-year-old woman was admitted to our hospital with rapidly progressive dyspnea for 3 days. On the day of admission, she was in severe respiratory distress with orthopnea. She had been diagnosed with hypertension 3 years earlier, which has been well controlled with medication. Her blood pressure was 110/70 mmHg; pulse, 135 beats/min; and respirations, 24 breaths/min. Cardiac auscultation revealed a grade III/VI diastolic murmur at the apex. The electrocardiogram showed sinus tachycardia. Chest radiography revealed bilateral pulmonary edema (Fig. 1). Laboratory studies were normal. A two-dimensional echocardiogram disclosed a large mass with a stalk on the posterior wall of the left atrium, measuring 4.5 × 3.4 cm (Fig. 2). The mass did not prolapse into the left ventricle, but extended into the mitral annulus and obstructed transmitral inflow. Color Doppler demonstrated flow turbulence across the mitral valve. Continuous-wave Doppler showed a severe mitral stenosis with a maximal velocity of 3.1 m/s and a mean pressure gradient of 20 mmHg through the mitral valve (Fig. 3).
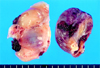
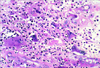
The operation was performed through a median sternotomy with a mild hypothermic cardiopulmonary bypass. Intraoperatively, two separate tumors were identified (Fig. 4). The main mass, observed on echocardiogram, originated from the posterior wall of the left atrium and extended into the pulmonary veins. The mass was 4 × 3.5 × 3.5 cm in size and dark red in color. The mass was excised and the posterior wall of left atrium was repaired. The second yellow mass, which was not detected by the echocardiogram, was attached to the interatrial septum and extended to the atrial aspect of the posterior mitral leaflet; it measured 5.5 × 3 × 1.5 cm in size. The tumor was almost completely excised, except for the small portion of mass on the posterior mitral leaflet. The defect of the interatrial septum secondary to the operation was repaired. We did not repair or replace the mitral leaflet. The macroscopic appearance of the main mass (Fig. 4, right side) was semi-solid and ball-shaped. The mass had a smooth outer surface and showed a homogenous appearance with a focal cystic change filled with a blood clot. The second mass (Fig. 4, left side) had a pinkish-yellow myxoid appearance with hemorrhagic spots and blood clots. Histologically, the tumor was composed of spindled or epithelioid pleomorphic cells with oval nuclei, prominent nucleoli, and abundant eosinophilic cytoplasm. In addition, intermixed giant cells were common. The neoplastic cells exhibited a high degree of nuclear pleomorphism and mitotic activity (Fig. 5). Focal necrosis was also present. On immunohistochemical staining, neoplastic cells showed positive immunoreactivity for vimentin and desmin but were negative for S-100 protein, CD34, CD31, smooth muscle actin, and cytokeratin. The histologic diagnosis was undifferentiated pleomorphic sarcoma. Postoperative metastatic work-up showed no evidence of metastasis. The patient did not receive chemotherapy or radiation and is still alive at present, 6 months after the operation
DISCUSSION
Primary malignant tumors of the heart are extremely uncommon,1,2 and almost all are sarcomas. There are several types of sarcomas, including angiosarcoma, rhadomyosarcoma, fibrous histiocytoma, spindle cell sarcoma, fibrosarcoma, synovial sarcoma, myxosarcoma, and unclassified sarcoma.5 Malignant fibrous histiocytoma is now regarded as synonymous with undifferentiated sarcoma.4 Undifferentiated pleomorphic sarcoma is a high-grade malignancy showing fibroblastic or myoblastic differentiation and areas of marked cellular pleomorphism. All primary tumors of the heart, whether malignant or benign, are potentially lethal because of intracavitary or valvular obstruction, peripheral embolization, and/or rhythm disturbances. Therefore, surgery should be performed as soon as possible after a cardiac tumor is found.6
Surgical resection of benign myxoma results in full recovery in most cases, whereas resection of malignant sarcoma leads to only palliation of the symptoms and does not contribute to long-term survival.7 Undifferentiated pleomorphic sarcomas proliferate rapidly, and generally patients die of progressive heart failure, although distant metastases are also encountered at diagnosis.8 The key diagnostic tool for cardiac tumors is transthoracic and transesophageal echocardiography. Typically, this diagnostic test accurately identifies the shape, size, possible valve involvement, and myocardial invasion of the tumor, thus providing information useful for determining the optimal therapeutic approach. However, it is difficult to determine the specific type of tumor from echocardiographic findings.
Previous studies have demonstrated that two types of consistency are detectable, even in benign myxomas, by two-dimensional echocardiography. Of 25 cases with atrial myxoma, 18 had a deformable and jelly-like echocardiographic appearance, whereas the others were non-deformable and firm.9 In the present case, the preoperative echocardiographic diagnosis was a benign myxoma, but histological and immunohistochemical studies revealed a malignant, undifferentiated pleomorphic sarcoma. Malignant fibrous histiocytoma tends to be located in the left atrium of the heart, most commonly on the posterior wall and/or interatrial septum.10-12 In a recent review, 38 (81%) of 47 cases were found in the left atrium.13 The majority of malignant fibrous histiocytomas develop in the left atrium and they more commonly arise along the posterior wall in comparison to the septum.10-12 Benign myxoma is usually a solitary tumor;6,14,15 however, undifferentiated cardiac sarcoma may form multiple masses.12,16-18
In conclusion, because the majority of cardiac undifferentiated pleomorphic sarcomas occur in the left atrium, these growths can be mistakenly diagnosed as benign myxoma preoperatively. However, careful echocardiographic preoperative evaluation, including tumor origin and multiple growth profile, may be helpful in identifying malignant cardiac tumors.



 XML Download
XML Download