

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Noncompaction of the ventricular myocardium (NVM) is a rare cardiac abnormality of unknown origin.1 It is characterized by prominent and excessive trabeculations in a ventricular wall segment with deep intertrabecular recesses perfused from the ventricular cavity. The condition is believed to be a cardiomyopathy caused by the arrest of normal embryogenesis in the endocardium and myocardium.2 Its common clinical presentation includes heart failure, ventricular tachyarrhythmia and thromboembolic events.3 It is also associated with other cardiac and extracardiac abnormalities.4 This is the first case of myocardial noncompaction and solitus ambiguous with polysplenia in an adult.
CASE REPORT
A 33-year-old man presented at the hospital with a three-month history of worsening chest pain and dyspnea upon exertion. He recalled being diagnosed with a congenital heart anomaly when he was eight years old, but he had not visited the hospital since then. He had no history of syncope or hypertension, and no family history of sudden cardiac death.
Upon his visit to the hospital, the patient's blood pressure was 110/60 mmHg, with a irregular pulse of 72 beats/min. Physical examination yielded irregular heart sounds without murmur. A 12-lead ECG revealed atrial fibrillation and T wave inversions in the V4-6 precordial leads and in the II, III, and aVF limb leads. Chest radiography revealed clear lung fields and no cardiomegaly. Laboratory tests revealed no significant abnormalities. Cardiac enzymes were found to be normal, and the laboratory data did not indicate inflammation.
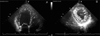
Echocardiography revealed an enlarged left ventricle (LV). The LV wall motion was consistent with severe global hypokinesia. LV systolic function was depressed (ejection fraction: 39%). Prominent trabeculations and deep intertrabecular recesses were observed on the short axis and apical views; the right ventricle was normal upon gross inspection. The noncompacted area examined involved mainly the anterior and inferolateral left ventricular segments, and the ratio of the noncompacted zone to the compacted zone was 2 : 3 (Fig. 1).
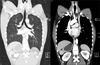
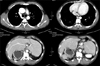
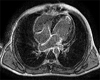
Based on the patient's past history, we checked the thoracoabdominal CT (multidetector row CT) for accompanied congenital anomalies. We found segmental thickening of the left ventricular (LV) myocardial wall consisting of two layers: a thin, compacted epicardial layer and an extremely thick endocardial layer with prominent trabeculations and deep recesses (Fig. 2), bilateral bilobed lungs with main bronchi below the pulmonary artery and no minor fissures, and double superior vena cava and left superior vena cava connections to the coronary sinus (Fig. 3). We also found persistent, accessory, azygous drainage to the intrahepatic vein and IVC segment, interruption of the inferior vena cava, a right-sided stomach, and multiple spleens in the right abdomen (Fig. 4). Cardiac magnetic resonance imaging (CMR) showed the two-layered structure of NVM, and revealed delayed enhancement of the trabeculations located at the apical portion of the LV, suggesting areas of fibrosis (Fig. 5). The coronary angiogram revealed normal coronary arteries. From this data, we diagnosed the patient as having left ventricular noncompaction, associated with situs ambiguous with polysplenia, and prescribed supportive care and medical treatment for LV dysfunction.
DISCUSSION
In the normal human hearts of children and adults, the left ventricle has up to three prominent trabeculations and is less trabeculated than the right ventricle. In humans, noncompaction of the ventricular myocardium (NVM) was first described in 1932, in a newborn upon autopsy.5 Since then, the rate of diagnosis of NVM has been steadily increasingly because of continuous improvements in imaging resolution quality and the awareness of echocardiographers. Several diagnostic criteria have been proposed for NVM, including a ratio of ≥ 2 for the wall thickness between the noncompacted trabeculated layer and the nontrabeculated compacted layer of the NVM at the end-systole, as measured along the parasternal short-axis.6,7
This abnormality is often associated with other congenital cardiac disorders, including coronary arterioventricular fistulae, ventricular septal defects, patent ductus arteriosus, atrial septal defects,8 a left coronary artery originating from the pulmonary artery,9 and dextrocardia.10 However, it is also occasionally encountered alone in the absence of other cardiac anomalies. It is also occasionally associated with extracardiac,4 particularly neuromuscular disorders.11
Situs ambiguous, or heterotaxia, is defined as the abnormal arrangement of organs and vessels, as opposed to the orderly arrangement typical of situs solitus or situs inversus. In contrast to individuals with situs solitus or situs ambiguous with dextrocardia, those with situs ambiguous have congenital heart disease in 50 - 100% of cases.12,13 The two major subcategories of situs ambiguous cases are situs ambiguous with polysplenia and situs ambiguous with asplenia.
Situs ambiguous with polysplenia (also known as left isomerism or bilateral left-sideness) is generally characterized by a midline of the abdominal organs and multiple spleens. There is no single anomaly that is pathognomonic for this condition. Affected patients have a lower prevalence of congenital heart disease (50 - 90%) and less severe defects than do those with situs ambiguous with asplenia.12,13
We think that this patient has a chance for a heart transplant in the future. For such a procedure, it is important to know about other noncardiac anomalies associated with noncompaction of the ventricular myocardium, especially vascular connections.
The delayed enhancement in the myocardium has been shown to increase under conditions of myocardial interstitial expansion.14 Previous histological studies have shown necrosis and fibrosis (interstitial expansion) in patients with NVM.3 These areas of fibrosis may potentially serve as a substrate for future lethal ventricular arrhythmias.15 We believe that cardiac magnetic resonance imaging (CMR) is a useful noninvasive diagnostic tool for the detection of myocardial fibrosis in patients with NVM.
To our knowledge, this is the first case report of a patient with situs ambiguous with polysplenia and noncompaction of the left ventricle.

 XML Download
XML Download