

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Congenital choledochal cysts are cystic or fusiform dilations of part of the common bile duct and are often accompanied by intrahepatic bile duct dilation. Occasionally, bile duct complications such as an aberrant bile duct and confluence of the left and right hepatic ducts into a dilated choledochal cyst are observed.1-4 Whether such abnormalities are associated with postoperative complications is of great concern. In order to ascertain this association, we investigated the image examination methods and clinical significance of patients with congenital choledochal cyst accompanied by intrahepatic bile duct dilatation and aberrant bile duct. In this study, we discuss the long-term efficacy and prognosis associated with the incorporation of relevant surgical methods into the standard surgical procedure to prevent postoperative complications.
MATERIALS AND METHODS
Patients
From January 1993 to Oct 2005, a total of 72 patients (1 male: 2.9 females) with congenital choledochal cysts were studied in the department of pediatric surgery at the Affiliated Hospital of Medical College, Qingdao University. The mean patient age was 3.5 years old, with a range from 15 days to 12 years. The major clinical symptoms were repeated episodes of abdominal pain (51/72), acute or chronic jaundice (35/72), white stool (13/72) and palpable abdominal mass (23/72). All diagnoses were confirmed during operation.
Imaging examination
Patients were diagnosed pre-surgically as having congenital choledochal cysts based on a survey of clinical symptoms, ultrasound examination and computerized tomography (CT) examination. It was determined whether there was evidence of accompanying intrahepatic bile duct dilation. For some patients, magnetic resonance cholangiopancreatography (MRCP), intravenous angiocholegraphy 3-D imaging and endoscopic retrograde cholangiopancreatography (ERCP) were employed to diagnose the existence of intra-hepatic bile duct dilation and pancreaticobiliary maljunction. Cholangiography was performed during the operation in all cases. When intrahepatic bile duct dilation was obvious, cholangiography, choledochoscope observation, and probing of intrahepatic bile ducts and the proximal end of the common bile duct at the junction with the biliary tract were performed together under direct observation during surgery. These diagnostic procedures were employed to assess the pathological changes in the common hepatic duct, cystic duct, left and right hepatic ducts and the pancreaticobiliary common duct, as well as to determine the extent of intrahepatic bile duct dilation and stenosis and whether any complicated bile duct malformation was present.
Follow-up
Complete follow-up data were collected in 51 cases. The postoperative condition of 31 of these patients was assessed in our hospital by physical examination and ultrasound or CT examination to investigate changes in the intra-hepatic bile ducts. MRCP was conducted in the patients presenting with additional bile duct malformations. For convenience, the remaining 17 patients were subjected to follow-up examinations via questionnaires after being examined in their local hospitals.
RESULTS
Surgical treatment of congenital choledochal cyst accompanied by intra-hepatic bile duct dilation.
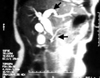
Of the 72 congenital choledochal cyst cases considered in this study, 22 (30.1%) had co-existing intrahepatic bile duct dilation of varying degrees. Twelve cases had cystic dilation of intra- hepatic bile ducts, 0.5-2.2 cm in diameter; these presented as cucurbit-like dilations in the left and/or right hepatic ducts, with valve-like, septum-like, or short tubiform stenosis at the opening to the common hepatic duct (Fig. 1A, B; 2, 3). The first procedure performed in each operation was resection of the dilated common bile duct and gall bladder. This was carried out as close to the porta hepatis as possible.
For the 12 cases in which intrahepatic or extrahepatic stenosis with proximal intrahepatic bile duct dilation was present, stenotic septum resection or a longitudinal incision at the stenosis and transverse suturing with 6-0 Dexson absorbable sutures was performed to alleviate the stenosis, followed by bile duct anaplasty. The other 10 cases presented with cone dilation that tapered from the beginning of the intrahepatic bile ducts, without evident stenosis at the proximal end of the common hepatic duct or the opening of the left and right hepatic ducts. Thus, further treatment was not required during these operations. Finally, in all cases, the intrahepatic bile ducts and the pancreaticobiliary common duct were flushed repeatedly and a subsequent Roux-Y hepatojejunostomy was performed.
Congenital choledochal cyst co-existing with aberrant bile duct and other complicated biliary malformations
In the 5 cases with co-existing aberrant bile ducts or other complicated bile duct malformations, specific surgical treatments were completed according to the particular condition for each patient. In one case, preoperative MRCP examination revealed that the left and right hepatic ducts merged into the common hepatic duct, which then converged at the dilated common bile duct, and another duct deriving from the sixth hepatic segment of the right lobe of the liver entered the cystic duct at the site adjacent to the common bile duct. It was confirmed during the operation that the aberrant bile duct derived from the lobes of liver had merged into the cystic duct directly, and that the aberrant bile duct was not connected with the major intra-hepatic biliary system as evidenced by operative cholangiography through the common hepatic duct. Because of abundant leakage of bile fluid from the aberrant bile duct, anastomosis between the aberrant bile duct and the common hepatic duct was indicated following excision of the common bile duct and gallbladder, and prior to Roux-Y hepato-jejunostomy (Fig. 4A, B).
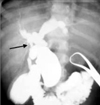
In another case, cholangiography during the operation revealed that where the left and right hepatic ducts entered the dilated choledochal cyst, they connected with the common hepatic duct and an aberrant bile duct deriving from the fifth hepatic segment of the right lobe of the liver. In this case, irrigation of the intrahepatic bile ducts demonstrated that the aberrant bile duct was connected with the major intra-hepatic biliary system. Therefore, ligation of the aberrant bile duct was performed before choledochoenterostomy (Fig. 5). In 3 other cases, the left and right hepatic ducts merged into the dilated choledochal cyst anastomosis of the right and left hepatic ducts respectively, as indicated by the long distance between the two openings after cyst resection at the superior position. Under these conditions, anastomosis is necessary to produce a common hepatic duct so that hepato-jejunostomy may be performed.
A total of 31 cases in this group achieved the desired pancreatocholangiography imaging during the operation, which revealed a long pancreaticobiliary common duct. A filling defect in the common pancreaticobiliary duct was observed in 5 cases, and was thought to be due to a silt-like pancreatic calculus in the pancreaticobiliary common duct. In these cases, irrigation of the pancreaticobiliary common duct resulted in a massive, white, cheese-like protein embolus being washed out from the end of the choledochous duct.
Surgical effects and long-term follow-up care
For 38 cases, complete follow-up data were collected. The follow-up period ranged from 6 months to 10 years, with a mean of 5.6 years. Post-surgical severe abdominal bleeding occurred in 2 cases, one of which was cured by conservative therapy of transfusion and hemostatic drugs and the other by surgical hemostasis. In addition, another patient suffered from slight biliary leakage and was cured by abdominal cavity drainage. In all other cases, no obvious complications were observed in the perioperative period and the patients were released from the hospital. Four patients complained of epigastric discomfort and abdominal pain, however these symptoms resolved without any special treatment; none of these four patients had an intrahepatic duct calculus. One patient underwent a secondary operation for adhesive intestinal obstruction 4 years after the choledochal cyst operation.
Postoperative change of intra-hepatic bile duct dilation
Postoperative ultrasound examination revealed intrahepatic biliary gas in 22 cases, suggesting that there may have been some reflux from the intestinal canal to the biliary tract that was not sufficient to induce evident biliary infection. The postoperative change in intrahepatic bile duct dilation was investigated by CT scan or ultrasound examination in 17 cases, with a follow-up period that ranged from 8 months to 8 years. For all cases the dilated intrahepatic bile duct was narrowed and some patients even recovered a normal diameter. The dilation was still obvious in 3 cases with severe cystic dilation of the intra-hepatic bile ducts, although it was markedly improved relative to the preoperative condition. No evidence of bile duct infection was apparent in these cases, suggesting that the radical treatment relieved the intra-hepatic bile duct dilation. In the cases that underwent aberrant bile duct anastomosis, postoperative MRCP examination showed that the anastomosis between the aberrant bile duct and the porta hepatis part of the common hepatic duct was in good condition and that bile flow was unimpeded.
DISCUSSION
It should be noted that recent research on the various mechanisms of bile duct carcinogenesis has revealed an association between bile duct cancer and pancreaticobiliary maljunction.5-8 Therefore, standard procedures such as cyst incision, pancreaticobiliary flow-division and hepatojejunostomy have been generally accepted. In clinical practice, 30-46% of congenital choledochal cyst cases are accompanied by intrahepatic bile duct dilation. Whether this abnormality of the intrahepatic bile ducts is associated with postoperative bile duct infection is a great concern.9 An improved understanding of pathological changes, diagnosis, and treatment has enabled steady progress in surgical techniques. Procedures including correction of stenosis at the proximal end of the intrahepatic bile duct, treatment of potential complicated bile duct malformations, and irrigation of the distal pancreaticobiliary common duct decrease the associated complications and contribute to the prognosis of the patients.
The incidence rate of intra-hepatic bile duct dilation in this group of choledochal cyst patients was 30.1%, and consisted mainly of two types. One was cone-shaped dilation that tapered from the common bile duct to the beginning of the intrahepatic bile duct, and the other was cystic dilation. Fifty-three percent of the cases in this study were of the cystic dilation type; among these the dilation occurred more frequently and obviously in the left lobe of the liver. Cystic dilated intrahepatic bile ducts were cucurbit-shaped, i.e., the intrahepatic bile duct was valve-like, septum-like, or of the short tubiform stenotic form, where the intra-hepatic duct merged into the common hepatic duct. If the intrahepatic bile duct stenosis was not relieved after cystectomy and hepatico-enterostomy, reflux into the intrahepatic bile duct could cause bile fluid retention and increase the possibility of reflux cholangitis and calculus formation. In this study, intrahepatic bile duct stenosis was relieved surgically and the incidence rate of postoperative bile duct complications was low, suggesting that the expanded treatment of intrahepatic bile duct stenosis could potentially reduce the incidence of postoperative complications.
The potential of intrahepatic bile duct stenosis should be considered for those with indications of intrahepatic bile duct dilation by ultrasound and CT scanning. Cholangiography, choledochoscope observation, probing of intrahepatic bile duct, and direct observation should be performed during the operation. Intrahepatic bile duct stenosis generally occurs at the confluence site of the left and right hepatic ducts. Such stenosis can be relieved by septum resection and a longitudinal incision combined with a transverse suture through the opening of the common hepatic duct. Many advanced diagnostic methods, such as 3-D spiral CT imaging, MRCP and 3-D magnetic resonance imaging (MRI), can be utilized to help develop a patient's surgical treatment plan.9-11 Before and during operation, there should be a careful investigation for any complications, such as a long pancreaticobiliary common duct, a potential tumor, intra-hepatic bile duct dilation, membrane-like stenosis, a biliary calculus, or a pancreatic calculus in the pancreaticobiliary common duct. If there is stenosis at the proximal end of common hepatic duct, the common hepatic duct should be resected above the stenosis, or the left and right hepatic ducts should be inosculated with the jejunum after being appropriately shaped. It has been found in clinical practice that even when many anti-reflux techniques are applied, biliary reflux may not be completely prevented. The fact that pneumobilia occurred in many cases in this study emphasizes this issue. However, most patients did not suffer from bile duct infection despite the existence of reflux. If there is no stenosis present at the anastomotic stoma or the proximal bile duct, any reflux substance can be discharged without retention and infection.10
The appearance of pancreaticobiliary maljunction varies with the type of choledochal cyst present, especially in association with cystic dilation and fusiform dilation. The distal end of the common bile duct should be resected without injuring the pancreaticobiliary common duct. In some cases, part of the cyst protrudes into the pancreas, and only through careful isolation can the distal end of the common bile duct be exposed. Therefore, imaging examination is especially important to identify maljunction of pancreatobiliary ducts.
Of the 5 unusual cases examined here, 2 were complicated by the presence of aberrant bile ducts, and in the other 3 cases, the left and right hepatic ducts were connected to the choledochal cyst. Aberrant bile ducts are thought to be the result of normal variation in biliary system development, and their incidence rate is relatively low (~5% of the normal population). Aberrant bile duct manifestations may include an additional duct connecting the liver to the common bile duct or the presence of an additional cystic duct besides the main biliary system, which normally includes the left and right hepatic ducts and the common hepatic duct. An additional aberrant duct may be connected with the main biliary system, or it may be a completely independent duct functioning to drain a portion of the bile flow. It has no clinical significance for the normal population; however, it is a significant complication for a congenital choledochal cyst. Oversight of the existence of an aberrant bile duct during the operation might lead to severe biliary leakage. Arbitrary ligation of the aberrant bile duct that was independently responsible for drainage of part of the bile flow will obstruct the corresponding intrahepatic bile duct and result in severe complications including liver cirrhosis and infection. Surgical anastomosis between an aberrant bile duct and the porta hepatis part of common hepatic duct was performed in one case of this group to avoid potential complications. Therefore, more attention should be paid to particular variations in bile duct formation. For the other 3 cases in which the left and right hepatic ducts were separately connected with the choledochal cyst, the cyst was excised entirely, and the left and right hepatic ducts were merged into one duct and then inosculated with the jejunum. In these cases, the cyst was completely resected and satisfactory long-term efficacy was obtained. An aberrant bile duct shares similar wall thickness and position with the left and right hepatic ducts; we therefore chose to perform anastomosis between the aberrant bile duct and the common hepatic duct prior to Roux-en-Y hepatojejunostomy. Postoperative MRI examination demonstrated that this procedure is practicable. If the jejunum had been inosculated with the very thin aberrant bile duct, stenosis would have been more likely to occur. This study demonstrates that the relevant surgical method should be incorporated into the standard surgical procedure to prevent postoperative complications associated with the treatment of congenital choledochal cyst.



 XML Download
XML Download