

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Hamartomatous polyps of the colon are rare in adults, and nearly all cases are associated with hereditary or familial polyposis syndromes.1-3 Colonic hamartomas are non-neoplastic lesions1, and these mucosal protuberances contain mesenchymal elements of excess vascular and/or fibrous stroma and glandular proliferation with cystic dilatation. Mesenchymal proliferation disorders are heterogeneous, and excessive growth may be a post-natal indication of an underlying developmental abnormality.4
Here, we report an unusual case of a giant colonic hamartoma in a 48-year-old man that is not associated with other hereditary or familial polyposis syndromes.
CASE REPORT
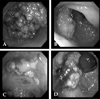
A 48-year-old man presented with a two-month history of weight loss and obstipation. He did not complain of diarrhea, hematochezia, or abdominal pain. There was no history of inflammatory bowel disease, skin disease, thyroid cancer, or genital cancer. He had no family history of inflammatory bowel disease or colon cancer. The results of his physical examination and laboratory tests were normal, and he did not show any verrucous lesions or pigmentation of the skin, alopecia, or onchyodystrophy. The patient subsequently underwent a colonoscopy, which revealed five sessile polyps, ranging from 1-2.5 cm in size in the descending and transverse colon. In addition, an obstructing mass was found in the proximal descending colon (Fig. 1). The initial endoscopic impression was that this mass represented a malignant lesion and multiple biopsies were performed. The multiple polyps in the descending and transverse colon were suspected to be colonic tumors. Biopsy analysis showed that the colonic polyps and the obstructing mass were sites of chronic inflammation, and they showed no signs of malignancy. CT scans showed no evidence of malignant disease in other organs. The patient underwent a total colectomy with ileorectal anastomosis, since the mass was causing luminal obstruction that resulted in obstipation and because multiple synchronous colon cancers were suspected. The gross specimen consisted of 135 cm of colon tissue. Six polypoid lesions were present in the transverse colon and descending colon. The largest polypoid lesion encircled the entire circumference of the transverse colon (Fig. 2). Microscopic examination showed that the polyps contained ramifying smooth muscle bands that arose from the muscularis mucosa. The smooth muscle bands were thick in the center of the polyp and thinner on the periphery, contributing to the polypoid appearance of the lesion. The surface epithelium was composed almost entirely of goblet and absorptive cells that appeared to be normal (Fig. 3). These features were consistent with a hamartomatous polyp. Postoperatively, the patient was examined using a duodenofiberscope and underwent a small bowel series. The results of these procedures showed no evidence of polypoid lesions.
DISCUSSION
Colonic hamartomas, or juvenile polyps, are acquired lesions most commonly found in individuals between 1 and 7 years of age. The lesions are usually associated with hereditary or familial polyposis syndromes. These colonic polyps are usually less than 4 cm in size, although larger polyps have been found.1 A MEDLINE search from 1966 to 2003 using hamartoma, colonic polyp, and giant hamartoma as search items was performed. After excluding hereditary and familial polyposis syndromes, only three relevant articles were found in English language journals. Colonic hamartoma, particularly of a large size and without mucocutaneous lesions, is rare and has been reported only twice.1,2 One report involved a 50-year-old man with ulcerative colitis. In this case, the lesion was located in the ascending colon and was approximately 5 cm in length. Resection was performed, because the large polypoid mass could not be distinguished from a possibly malignant mass.2 The other case involved a 26-year-old man with multiple large bowel polyps and a single immense colonic Peutz-Jeghers polyp.1 An endoscopic biopsy showed this to be an inflammatory polyp. The lesion was postoperatively diagnosed as a hamartoma. In the present case, the hamartoma occurred in a middle-aged man who had normal colonic mucosa. Additional multiple hamartomatous polyps were later found to be distributed along the entire colon. This case was not associated with hereditary or familial polyposis syndromes. Preoperatively, we diagnosed the case as multiple colonic carcinomas based on the endoscopic observation, and because cancer could not be diagnostically excluded due to the patient's age. In addition, resection was required because of luminal obstruction.
Colonic hamartomas are non-neoplastic lesions composed of localized, disorganized overgrowths of normal mature tissues. In one rare case, an adenocarcinoma was reported to have arisen from a hamartomatous polyp.5 Although the lesion is rarely associated with cancer, endoscopic or surgical removal seems prudent, particularly if the lesion grossly resembles a villous polyp, which is associated with a high incidence of cancer. Another argument for lesion removal is the impossibility of differentiating between an adenoma and a hamartoma in small biopsy specimens.
In summary, multiple giant hamartomas of the colon that are not associated with hereditary or familial polyposis syndromes are rarely encountered in adults. Only two previous cases have been reported in the medical literature. Hamartomas can be large in size and may simulate a malignant lesion. As in the present case, endoscopic biopsies may not be definitive in the diagnosis of hamartoma, and resection may be required for an accurate diagnosis and for the relief of obstruction. For this case, continuous follow-up is required to monitor the symptom that has not been appeared.


 XML Download
XML Download