

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
The proportion of colorectal cancer has been gradually increasing during the past several decades in Korea. In 1980, when the Central Cancer Registry began, colorectal cancers accounted for 5.8% of total cancers.1 In 1990 and 2002, this figure increased to 6.9% and 11.2%, respectively. With estimates of 11,000 new cases annually, colorectal cancer is the fourth most common cancer and the fourth leading cause of cancer-related deaths in Korea.1,2 In 1983, the death rate of colorectal cancers accounted for 1.6 per 100,000 person-years, and rapidly increased to 10.6 per 100,000 person-years in 2002.2
Considerable studies have examined factors that influence the development of colorectal cancer. Family histories of colorectal cancer,3 obesity,4 animal fat intake,5 alcohol,6 cigarette smoking,7 physical inactivity,8 and insulin resistance9 have been regarded as predisposing factors of colorectal cancer.
Increasing evidence suggests that inflammation may be linked to the pathogenesis of colorectal cancer. Many studies have suggested a relationship between colorectal cancer and chronic inflammation. The risk of colorectal cancer increases in patients with long-standing inflammatory bowel diseases.10 In addition, several studies have consistently shown a risk reduction for the incidence of colorectal adenoma and cancer among regular and prolonged users of aspirin or other non-steroidal anti-inflammatory drugs (NSAIDs).11,12 However, two conflicting observational results were recently reported on the relationship between the inflammatory marker C-reactive protein (CRP) and the risk of colorectal cancer. A nested case-control study showed that individuals with CRP concentrations in the highest quartile had a significantly higher risk for the incidence of colon cancer compared with individuals in the lowest quartile.13 In contrast, another prospective study demonstrated that an elevated plasma CRP level was not a predictor of colorectal cancer but was merely increased after the onset of colorectal cancer.14
White blood cell count (WBC) is another marker of nonspecific inflammation and was analyzed in this study to examine its relationship with the risk of colorectal cancer. We hypothesized that an elevated WBC is associated with the risk of colorectal cancer. Furthermore, WBCs and CRP levels tend to be chronically elevated in smokers. Therefore, we also hypothesized that the association between inflammation and risk of colon cancer would be independent of smoking.15,16 To test these hypotheses, we prospectively determined the risk of colorectal cancer associated with WBC.
MATERIALS AND METHODS
Study population
The Korean Cancer Prevention Study (KCPS) is a prospective cohort study that was designed to assess risk factors for mortality, incidence, and hospital admission for cancer. The KCPS cohort was composed of government employees, teachers, and their dependents insured by the Korean Medical Insurance Corporation from 1992 through 1995. The subjects had at least one medical examination and completed a questionnaire during that period. The KCPS cohort includes 1,329,525 Koreans (846,907 men and 482,618 women) from 30 to 95 years old who met the above selection criteria. The current analysis was limited to the 446,878 participants who were the insured workers' family dependents in 1993 and 1995. Insured workers were excluded from this study population because there was no WBC record in their examinations. The 3,703 participants who reported a history of any cancer at enrollment and 1,483 participants who died of cancer before the start of follow-up were also excluded. Additionally, 17,273 participants with missing data on any covariate information were excluded from the study. After these exclusions, 424,419 participants (108,907 men and 315,512 women) who received medical examination in 1993 and 1995 were included in the analyses.
Data collection
Medical examinations were performed according to a standard procedure and conducted by the medical staffs at local hospitals. In the 1993 and 1995 questionnaires, participants were asked about smoking habits and other health behaviors. Participants were also asked if they were currently being treated for cancer or other diseases. If so, they were asked for the date of diagnosis. The completed questionnaires were reviewed by trained staff and then entered into a database. The data were also checked and cleaned again during the analysis. Body mass index (BMI, kg/m2) was calculated as the ratio of weight (kg) divided by height squared (m2). WBC, plasma glucose, and total cholesterol were measured under fasting conditions for routine clinical purposes. Each hospital had internal and external quality control procedures directed by the Korean Association of Laboratory Quality Control. Alcohol consumption per day was categorized as follows: no drinking (0 g), light drinking (1-29.9 g), and moderate to heavy drinking (30 g or more). Diabetes was defined as self-reported history of the disorder or when a fasting plasma glucose level was ≥ 126 mg/dL. Hypertension was defined as self-reported history of the disorder or when systolic blood pressure was ≥ 140 mmHg or diastolic blood pressure ≥ 90 mmHg.
The maximum follow-up period was 10 years, from January 1, 1994 to December 31, 2003. The exact dates of completion of the survey form were not recorded. Consequently, follow-up accrual began January 1 of the calendar year and ended in the year in which the survey form was completed. Subjects who completed a survey but died in the same calendar year were excluded.
Because the study involved routinely collected medical data, it was not necessary to obtain individual participant consent. The study was approved by both Institutional Review Boards of Yonsei University and the Johns Hopkins Bloomberg School of Public Health.
Cancer outcomes
The primary outcomes were mortality and incidence risk of colon and rectal cancers based on the National Cancer Registry data and hospitalization records. Although Korea has a National Cancer Registry, reporting may not have been complete during the follow-up period. Thus, hospital administration files were used to identify the date of diagnosis. Therefore, incident cancer cases were coded as occurring either upon registration with the National Cancer Registry or upon hospital admission due to cancer diagnosis. Mortality was ascertained from death certificates. A computerized search of death certificate data from the National Statistical Office in Korea was performed using the unique identification number assigned at birth. Causes of death were assigned at the hospitals by trained abstractors. The analysis was limited to those deaths assigned to the 10th revision of the International Classification of Diseases (ICD-10): C18, malignant neoplasm of colon; C19, malignant neoplasm of rectosigmoid junction; and C20, malignant neoplasm of rectum.
Statistical analysis
Based on WBC at enrollment, Chi-square tests and one-way analyses of variance were used to analyze the statistical differences among characteristics of the study participants. Categorization of WBC into quartiles was based on the distribution of WBC among the study participants aged 40 to 95 years at baseline. Therefore, WBC (cells/µL) quartiles were categorized as ≤ 5500, 5501-6500, 6501-7600, and > 7600. In all primary analyses, the WBC quartile of ≤ 5500 cells/µL was used as the reference group.
Age-adjusted death and incidence rates were calculated for each WBC quartile and were directly standardized to the age distribution of the Korean population in 1995. Cox proportional hazards regression models were used to compute hazard ratios (HR) and their 95% confidence intervals (CIs), while adjusting for other potential risk factors. Cox models were also used to assess the trends in risk with quartiles of WBC as a continuous variable. To exclude sub-clinical disease at baseline, we conducted analysis for the incidence of colon cancer after excluding cases that occurred within 2 years of follow-up. The association between WBC and the incidence of colon cancer was also assessed by stratification according to smoking status in order to confirm that the association was independent of the effects of smoking on WBC.
All analyses were conducted using SAS statistical software, version 8.1 (SAS Institute Inc, Cary, NC, USA). All statistical tests were two-sided, and statistical significance was determined at p < 0.05.
RESULTS
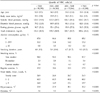
The baseline characteristics of the study population (according to WBC quartiles) are shown in Tables 1 and 2. Increased mean BMI, systolic and diastolic blood pressure, fasting plasma glucose concentration, total cholesterol concentration, amount of daily alcohol consumption, smoking duration, and frequency of meat intake all correlated with higher WBC. The percentages of hypertension, diabetes, and current smokers also correlated with WBC. Regular exercise was inversely associated with WBC.
During the 10 year follow-up, 25,458 and 21,482 deaths occurred among men and women, respectively. The multivariate adjusted HRs for all-cause mortality in the highest WBC quartile were 1.15 and 1.22 compared with the reference category in men (95% CI 1.11-1.20, p for trend < 0.0001) and women (95% CI 1.18-1.27, p for trend < 0.0001), respectively (Tables 3, 4).
For men, there were 9,010 deaths from all cancers, including 310 from colon cancer and 229 from rectal cancer, during the 10 year follow-up. For women, there were 5,871 deaths from all cancers, including 352 from colon cancer and 237 from rectal cancer. Tables 3 and 4 show that HRs for mortality from colon cancer increase with WBC quartiles among men and women. In men, the multivariate adjusted HRs for all-cause mortality in the highest WBC quartile were 1.33 (95% CI 1.03-1.72, p for trend = 0.0031) for colorectal cancer and 1.55 (95% CI 1.10-2.18, p for trend = 0.0014) for colon cancer, compared with the reference category (Table 3). The higher mortality risk associated with higher WBC quartiles was also observed for colon cancer in women (highest versus lowest quartile: HR 1.51, 95% CI 1.12-2.03, p for trend = 0.0049) (Table 4). In contrast to colon cancer, there was no significant difference in mortality risk for rectal cancer between the highest quartile and the lowest quartile in men or women.
The incidences of colon cancer during the 10 year follow-up were 604 among men and 838 among women. The trend of colorectal cancer incidence was generally similar to the mortality risk of colorectal cancer. Tables 5 and 6 show that HRs for colon cancer incidence increase with WBC quartile. The multivariate adjusted HRs for incidence in the highest WBC quartile were 1.23 (95% CI 1.03-1.47, p for trend = 0.0030) for colorectal cancer and 1.38 (95% CI 1.09-1.76, p for trend = 0.0017) for colon cancer, compared with the reference category in men (Table 6). The higher incidence risk associated with an increased WBC was also seen for colon cancer in women (highest versus lowest quartile: HR 1.46, 95% CI 1.20-1.78, p for trend = 0.0003) (Table 6). There was no significant difference in incidence risk for rectal cancer between the highest quartile and the lowest quartile among men or women. A total 145 cases of colon cancer occurred within 2 years of follow-up, 61 cases for men and 84 cases for women. Even after excluding these cases that occurred within 2 years of follow-up, the association between WBC and colon cancer was sustained. The multivariate adjusted HRs for incidence of colon cancer in the highest WBC quartile were 1.34 (95% CI 1.04-1.73, p for trend = 0.0058) in men and 1.41 (95% CI 1.14-1.73, p for trend = 0.0058) in women.
We also assessed the association between WBC and incidence of colon cancer after stratification by smoking status (non-smokers, ex-smokers, and current smokers) in order to confirm that the associations were independent of the effects of smoking on WBC.
Among men who reported having never smoked, a positive linear trend was observed between the incidence of colon cancer and WBC. The multivariate adjusted HRs for incidence of colon cancer were 1.56 (95% CI 0.83-2.95), 2.61 (95% CI 1.45-4.68), and 2.90 (95% CI 1.62-5.17) with increasing WBC quartiles, compared with the reference quartile (p for trend < 0.0001) (Fig. 1). A similar positive linear trend was also observed in female non-smokers. The multivariate adjusted HRs for colon cancer incidence were 1.27 (95% CI 1.04-1.55), 1.26 (95% CI 1.02-1.55), 1.47 (95% CI 1.19-1.81) with increasing WBC quartiles, compared with the reference quartile (p for trend = 0.0006) (Fig. 2). However, there was no significant difference in incidence of colon cancer among ex-smokers and current smokers (Fig. 1, 2).
DISCUSSION
In this large prospective cohort study of Korean men and women, a positive association between WBC and the risk of colon cancer was found. Our data suggest that an elevated WBC increases the incidence risk and mortality of colon cancer in men and women. These findings are consistent with emerging evidence suggesting that inflammation increases the risk of colon cancer. Individuals with long-term inflammatory bowel disease, in particular ulcerative colitis, are at higher risk for developing colorectal cancer than ordinary individuals.10 A clinical trial demonstrated that regular use of anti-inflammatory agents can reduce the risk of colorectal adenoma, a well-known precancerous lesion.17 In a recent prospective cohort study examining the association between WBC and the mortality risk of cancer, an elevated WBC correlated with an increased mortality risk for all cancers. However, the study failed to show this association through subgroup analyses of colon, breast, or prostate cancers.18 This may be due to the lower number of deaths from the site-specific cancers mentioned.
There are two previous prospective studies with conflicting results on the relationship between inflammatory markers and the incidence of colorectal cancer. One study was a nested case-control prospective study of 172 colorectal cases (131 colon cases, 41 rectal cases) from the CLUE II cohort of 22,887 residents from Washington County, Maryland. In this study, the incidence risk of colon cancer increased with CRP levels. However, this association was not found in rectal cancer.13 In the other study, using 27,913 healthy women within the Women's Health Study, high CRP levels were not a predictive risk factor for the development of colorectal cancer.14
Despite a positive association between WBC and the incidence risk and mortality of colon cancer, we did not find a similarly significant association with rectal cancer in the present study. A potential limitation of the CLUE II cohort study is the relatively small number of rectal cancer patients (n = 41), which could have weakened the association between an elevated CRP level and the incidence of rectal cancer. Our study overcomes this weakness by conducting prospective follow-ups on a larger number of rectal cancer patients during a 10 year period. Our findings imply that the role of inflammation in the development of colon cancer may be different from that of rectal cancer. The biological mechanisms through which elevated WBC increases the risk of colon cancer have not yet been established. However, several plausible mechanisms between colon cancer and inflammation deserve consideration based on previous studies. Cyclooxygenase-2 (COX-2) may be linked to the pathogenesis of colon cancer. COX-2 protein is over-expressed and prostaglandin E2 levels are elevated in the portal vein and colonic mucosa in human colorectal cancers.19,20 COX-2 may control angiogenesis by modulating production of the vascular endothelial growth factor, which promotes sustained endothelial cell proliferation and vascular permeability during tumorogenesis.21,22 Many studies also demonstrate that the carcinogenic effect of inflammation may be linked to DNA damage in proliferative cells by oxygen radicals,23 alteration of p53 tumor suppressor gene,24 or inhibition of apoptosis.25 Dietary and lifestyle risk factors for colon cancer, such as a diet high in calories, animal fat and/or refined carbohydrates, physical inactivity, central obesity, and high body mass index are also related to inflammation and insulin resistance.26,27 Insulin resistance may lead to tumor growth by elevating bioavailable insulin growth factor-1 and decreasing insulin growth factor binding protein-1.28 These inflammatory effects on colon cancer may not only be through systemic pathways, mediated by cytokines and chemokines, but may also be directly linked to the colonic epithelium. A recent study shows that individuals with more risk factors for colorectal cancer have a higher level of calprotectin, which is a marker of bowel inflammation at the tissue level.29
Our study has several potential limitations. First, WBCs during the 10 year follow-up were not available for our study. Thus, only one measurement of WBC, at baseline examination, was included in the analysis. Therefore, it was not possible to determine whether an acute, brief episode of inflammation or chronic inflammation was responsible for the correlation found in the current study. Second, data on potentially confounding factors, such as a history of inflammatory bowel disease, colorectal polyps, or medicinal use (aspirin, other NSAIDs, or estrogen use) were unavailable in the baseline questionnaire. These variables are not fully adjusted in our Cox-proportional hazards regression model. Lastly, the cohort population, particularly the older population, might not be representative of the general Korean population.
Despite these potential limitations, the current study has several important strengths. First, our study is a large prospective study with a relatively long follow-up period, so we can be confident about the temporal relationship between inflammation and the risk of colon cancer. Second, this positive association was sustained even after excluding cases of colon cancer that developed within the first 2 years of follow-up, thereby reducing the likelihood of a subclinical cancer at baseline. Consequently, elevated WBC was unlikely to be caused and biased by subclinical colon cancer. Finally, similar positive trends observed in non-smokers suggest that the incidence risk of colon cancer, associated with an elevated WBC, is independent of the effects of smoking on WBC.
In conclusion, our findings demonstrate that elevated WBC is a predictor of the incidence risk and mortality of colon cancer. These results support our hypothesis that inflammation increases the risk of colon cancer. Further observational and experimental studies are needed to confirm these findings and to determine the role of inflammation in the carcinogenesis of colon and rectal cancer.







 XML Download
XML Download