

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Alarming rises in the prevalence of certain pathogenic bacteria resistant to some antimicrobial agents has been noted worldwide. Antimicrobial selective pressures, which are the primary determining factors of the prevalence of resistant bacteria, differ significantly depending on the region and time. Therefore, monitoring resistance is necessary for empirical selection of the most appropriate antimicrobial agents to treat infected patients. Monitoring temporal trends of resistance is considered most beneficial for the detection of subtle changes in resistance.1
Antimicrobial resistance surveillance is also necessary to assess the extent of problems and determine the need for intervention.2 Alexander, PROTEKT, SENTRY, and other programs3,4 are good examples conducted internationally by collecting strains and testing by a reference laboratory. For example it was believed that the Alexander project had provided a resource for measuring trends in the susceptibility patterns of respiratory pathogens at the national, regional and global levels.4 These type programs can provide the most accurate information. However, they are very costly. Analysis of routine susceptibility test data at hospitals has inherent inaccuracies due to differences in methodology and interpretation, but does not require many additional resources.3,5
The KONSAR program in Korea was initiated in 1997,6 based on a World Health Organization recommendation. Two surveillance methods have been used, which include the analysis of hospital-tested data, and the testing of collected strains by the coordinating laboratory. Analysis of test data in 20037 revealed a further increase of vancomycin-resistant Enterococcus faecium, fluoroquinolone-resistant Klebsiella pneumoniae, and imipenem-resistant Acinetobacter spp. The previous second program revealed wide dissemination of metallo-β-lactamase (MBL)-producing Acinetobacter spp. and Pseudomonas spp.,8 and plasmid-mediated CMY-2 and DHA-1 allele-positive Escherichia coli and K. pneumoniae.9
Currently, more problematic antimicrobial agent-organism combinations worldwide include methicillin-resistant Staphylococcus, vancomycin-resistant E. faecium, expanded-spectrum cephalosporin-resistant K. pneumoniae,10 multidrug resistant (MDR) Acinetobacter spp.11 and imipenem-resistant Pseudomonas aeruginosa.12
The resistance rates of nosocomially-acquired bacteria are generally higher than those of community-acquired ones, necessitating differentiation of these two groups in the analysis. Yet, it is sometimes difficult to separate them satisfactorily. In the previous KONSAR program, data were collected from hospitals only, but in 2003, data were also collected from a commercial laboratory, which tested a large number of specimens which were submitted mostly from primary-care clinics in many parts of Korea.7
In the analysis of resistance data, NCCLS13 recommends inclusion of the first isolate of a given species per patient per analysis period (e.g., year), irrespective of the antimicrobial susceptibility profile or other phenotypic characteristics. When multiple isolates of nosocomial pathogens from a patient are included, resistance rates become significantly higher, but elimination of duplicate isolates may result in the underestimation of resistance rates and mask trends in emerging resistance.5
In this study susceptibility test data generated by the KONSAR group hospitals were analyzed, and the resistance rates at hospitals were compared to those at a commercial laboratory. In addition, the effects of excluding duplicate isolates of some selected species on resistance rates were analyzed using test data from the coordinating laboratory.
MATERIALS AND METHODS
Routine susceptibility test data on common aerobic bacteria isolated in 2004 were collected from 44 KONSAR group hospitals located both in large cities and in small provincial cities throughout Korea. Data were also obtained from one commercial laboratory, which tested specimens received mostly from primary clinics in many parts of the country. The data from eight hospitals were excluded from the analysis due to poor performance versus the WHO/CDC quality control program. Data were also excluded from the analysis when the numbers of isolates in a hospital were less than 10 for non-typhoidal Salmonella, or less than 20 for other species.
Three hospital groups, which were determined based on the location and bed capacity at the time of initiation of the program (≥ 1000 beds countrywide, < 1000 beds in Seoul, and < 1000 beds in non-Seoul), were used to compare mean resistance rates, despite changes in bed capacity at some hospitals.
As in the previous study, the mean resistance rates in each hospital groups were calculated from the resistance rates at each hospital to minimize the influence of a large numbers of isolates at some hospitals.3,14 The data from the commercial laboratory were analyzed separately. Resistance rates, which did not include intermediate susceptibility, were calculated from all isolates, including duplicate ones. The effect of excluding duplicate isolates on the resistance rates was analyzed for some antimicrobial-species combinations using the WHONET 5 program.15 Statistical significance of resistance trend was not determined as it was the common practice in the large scale continuous surveillance program.4,16
RESULTS
Rank order of isolates and methods of susceptibility testing
The number of isolates at hospitals in 2004 increased slightly compared to those in 2003, but the rank order remained the same in all 13 organisms (Table 1). The most prevalent species in hospitals was Staphylococcus aureus (20.2%), however it was E. coli (29.7%) at the commercial laboratory. The proportions of E. faecium to all isolates of E. faecalis plus E. faecium were 47.2% in hospitals and 24.9% at the commercial laboratory.
The responses to our questionnaire showed that the susceptibility test methods used for E. coli and S. aureus were the NCCLS disk diffusion method by 10 and 13 hospitals, the broth microdilution method (Vitek [bioMerieux, Marcy l'Etoile, France] or MicroScan [Dade MicroScan Inc., West Sacramento, CA, U.S.A.] system) by 21 and 17 hospitals, and a combination of the two by one and two hospitals, respectively. The fluoroquinolone susceptibility of gram-negative bacilli was mostly tested using ciprofloxacin, but some hospitals used levofloxacin instead. Kinds of antimicrobial agents used to test the susceptibility of E. coli and S. aureus were similar to those used in 2003 (data not shown).
Resistance rates of hospital isolates
The present surveillance showed that the mean oxacillin resistance rates of S. aureus and coagulase-negative staphylococci (CNS) in hospitals were 68% and 73%, respectively (Table 2). The resistance rate of S. aureus was much higher than that of CNS to fluoroquinolone (60% vs. 35%), but lower to cotrimoxazole (20% vs. 35%). Of Streptococcus pneumoniae tested, 68% were oxacillin-screening test positive, suggesting penicillin nonsusceptibility. The ampicillin resistance rate of E. faecalis was 2% in this study. Ampicillin and vancomycin resistance rates of E. faecium were 90% and 25%, respectively.
The resistance rates of E. coli to cefotaxime and K. pneumoniae to ceftazidime were 14% and 34%, respectively (Table 3). The resistance rates of E. coli and K. pneumoniae to cefoxitin were 8% and 32%, respectively (Table 3). The lowest resistance rates to cephalosporins shown by Enterobacter cloacae and Serratia marcescens were to cefepime, 8% and 17%, respectively. Imipenem-resistant E. coli, K. pneumoniae, E. cloacae and S. marcescens isolates existed, although the rates were very low (Table 3).
The resistance rates of Acinetobacter spp. were lower to imipenem (17%) and cefoperazone-sulbactam (19%) than to other antimicrobial agents, and those of P. aeruginosa were lower to ceftazidime (19%), and meropenem (20%), but slightly higher to imipenem (24%).
The resistance rates to gentamicin and tobramycin in this study were relatively high: in E. coli 24% and 20%, respectively, and in K. pneumoniae 26% and 36%, respectively. Amikacin resistance rates were 10% to 46%, except for E. coli (Table 3). E. cloacae was the species with the lowest resistance rate to fluoroquinolone, 11%, while Acinetobacter spp. was the species with the highest resistance rate of 56%.
The resistance rates of nontyphoidal Salmonella to ampicillin, cotrimoxazole, and fluoroquinolone were 44%, 7% and 0.7%, respectively (data not shown). Among the Haemophilus influenzae isolates 47% were resistant to ampicillin and 51% produced β-lactamase.
Resistance rates of commercial laboratory-tested isolates
The resistance rates of S. aureus to oxacillin (58%) and gentamicin (54%), and those of E. faecium to ampicillin (78%), fluoroquinolone (69%), and vancomycin (11%) at the commercial laboratory were lower than those in hospitals (Table 2). A comparison of the resistance rates of the commercial laboratory-tested gram-negative bacilli to those of hospital isolates showed that the cefotaxime resistance rates of E. coli were 12% and 14%, respectively, and cefoxitin resistance rates of K. pneumoniae were both 32%. However, cefotaxime, ticarcillin-clavulanic acid, and amikacin resistance rates of E. cloacae and S. marcescens were much lower. The imipenem and meropenem resistance rates of P. aeruginosa, 13% and 15%, respectively, were only slightly lower than those found in hospitals, but resistance rates of Acinetobacter spp., 6% and 11%, respectively, were much lower (Table 3).
The E. coli isolates tested by the commercial laboratory, and those by the hospitals, showed similar fluoroquinolone resistance rates, 33% and 32%, respectively. It is interesting to note that the commercial laboratory-tested Acinetobacter spp. and P. aeruginosa showed higher fluoroquinolone resistance rates than hospital isolates (Table 3).
Trends of significant resistance
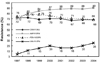
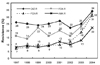
The prevalence of oxacillin-resistant S. aureus and penicillin-nonsusceptible S. pneumoniae remained similar, but a further increase of ampicillin- and vancomycin-resistant E. faecium was observed (Fig. 1). The resistance rates of K. pneumoniae to ceftazidime, cefoxitin, fluoroquinolone and amikacin also increased (Fig. 2).
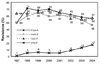
Acinetobacter spp. showed a slight downward trend in resistance to fluoroquinolone, amikacin, and ceftazidime, but a steady upward trend in resistance to imipenem (Fig. 3). In the comparison of the resistance trends of the isolates in 2003 and 2004, the resistance rates to all three aminoglycosides, and to some β-lactams, decreased slightly, but the resistance to imipenem and cefoperazone-sulbactam was slightly increased (Fig. 4).
In the comparison of resistance rates by hospital groups, isolates of vancomycin-resistant E. faecium, fluoroquinolone-resitant E. coli, cefoxitin-resistant K. pneumoniae, imipenem-resistant P. aeruginosa and Acinetobacter spp. were relatively more prevalent at the large hospital group than at the medium-size hospital group (Fig. 5). At the commercial laboratory, the rates of vancomycin-resistant E. faecium, imipenem-resistant P. aeruginosa and Acinetobacter spp. were lower, but the rate of fluoroquinolone-resistant E. coli was similar.
Resistance rates excluding duplicate isolates
Coordinating laboratory data showed that the resistance rates including all isolates were more than 5% higher compared to those including only the first isolate from a patient in oxacillin-resistant S. aureus, vancomycin-resistant E. faecium fluoroquinolone-resistant E. coli, ceftazidime-resistant K. pneumoniae, piperacillin- and imipenem-resistant P. aeruginosa (Fig. 6). The data from the coordinating laboratory were used to determine the time (day) between the first isolation of an imipenem-susceptible strain and the subsequent isolation of an imipenem-resistant strain of P. aeruginosa from same patients. The first resistant strain was detected within 4 weeks in 58 of 78 (74%) patients (Fig. 7). This suggested that, even in the monthly analysis of resistance rates, including the susceptibility of only the first isolate may result in the underestimation of the prevalence of some other resistances.
DISCUSSION
A comparison of total number of isolates tested in 2004 vs. 2003 showed a slight increase at hospitals, whereas there had been a significant decrease at the commercial laboratory (Table 1). The rank order remained the same for all 13 organisms in hospitals, but at the commercial laboratory, K. pneumoniae moved from the fifth to the fourth most prevalent, and coagulase-negative staphylococci dropped from the fourth to the fifth most prevalent.7
Kinds of antimicrobial agents used to test susceptibility of E. coli and S. aureus did not change significantly compared to those in 2003. With the increasing prevalence of CTX-M type extended-spectrum β-lactamase (ESBL) in Korea, testing the susceptibility of E. coli, K. pneumoniae and Proteus mirabilis to at least ceftazidime and cefotaxime became necessary for optimal detection of the enzymes,17 but not all hospitals tested susceptibility to both of these antimicrobial agents.
The mean oxacillin resistance rates of S. aureus and coagulase-negative staphylococci (CNS) in hospitals were 68% and 73%, respectively (Table 2). Oxacillin-resistant S. aureus is now highly prevalent, not only in Japan,18 but in other countries as well. Over 40% of S. aureus isolates in Greece, Italy, and United Kingdom were oxacillin-resistant, according to a surveillance study in 1999-2002.19 The penicillin G breakpoint for Streptococcus pneumoniae is for the treatment of meningitis. A high penicillin G non-susceptible rate of pneumococci by oxacillin-disk screening test (68%) in this study suggests that empirical selection of penicillin G, without susceptibility testing, may result in a high rate of clinical failure in the treatment of meningitis. Penicillin-non-susceptible pneumococci are very prevalent in some other Asian countries, as well,20 and increased penicillin resistance was also reported in the United States in the 1990s.21
The proportion of ampicillin-resistant E. faecalis was 2% in this study. Ampicillin-resistant E. faecalis was considered to be a misidentification of E. faecium in surveillance of the United Kingdom.22 A thorough review of other unexpected antibiograms, such as < 100% vancomycin susceptibility for S. aureus, < 100% imipenem susceptibility for Escherichia coli, and > 0% ampicillin susceptibility for K. pneumoniae, was also recommended to improve the quality of surveillance data.23 The vancomycin resistance rate of E. faecium was 25%. Difficulty in the control of vancomycin-resistant enterococci was shown by a high prevalence at a Chicago hospital,24 where the proportion of vancomycin-resistant E. faecium isolates increased from 28.9% to 72.4%, between 1993 and 2002.
The resistance rates of E. coli to cefotaxime and K. pneumoniae to ceftazidime were 14% and 34%, respectively (Table 3). E. coli and K. pneumoniae often acquire ESBL genes. In Korea, TEM-, SHV-, CTX-M-type ESBLs were reported.25-27 An analysis of K. pneumoniae strains collected between 1998 and 2002 from Asian countries28 showed that ESBL-producing isolates were particularly prevalent in Singapore (35.6%), China (30.7%), and the Philippines (21.9%). Increased prevalence of ESBL-producing E. coli and Klebsiella spp. over time was also reported in Europe.29
The cefoxitin resistance rate of K. pneumoniae was 32% (Table 3). A majority of the resistant isolates likely produced plasmid-mediated AmpC β-lactamases. DHA-1 and CMY-2 enzymes were reported to be the prevalent plasmid-mediated AmpC enzymes in Korea.9,30,31 Dissemination of E. coli and K. pneumoniae strains producing plasmid-mediated AmpC β-lactamases has become a worldwide problem,32 since the enzymes confer resistance not only to cephalosporins and cephamycins, but also to carbapenems when the mechanism is combined with porin loss.33
Imipenem-resistant E. coli, K. pneumoniae, E. cloacae and S. marcescens isolates existed, although the rates were very low (Table 3). MBL-producing E. cloacae,34,35 and S. marcescens and Citrobacter freundii35 were reported in Korea. The resistance rates of Acinetobacter spp. were lower to imipenem (17%) and cefoperazone-sulbactam (19%) than to other antimicrobial agents. Higgins et al.36 reported that in vitro activity of β-lactam-β-lactamase inhibitor combinations against A. baumannii are mainly determined by the intrinsic activity of the inhibitors alone. It was reported that sulbactam has a good intrinsic activity against MDR Acinetobacter strains at concentrations readily achievable in human serum and may therefore have some therapeutic implications in the treatment of infections caused by MDR A. baumannii infections. Smolyakov et al.37 reported that ampicillin-sulbactam appeared to be one of the last effective and safe empirical resorts for the treatment of MDR A. baumannii bloodstream infections, but in our present study, the resistance rate to this combination was not low (40%).
Increasing resistance of P. aeruginosa and Acinetobacter spp. to carbapenems is the most serious problem, as it is the only class of β-lactam active against ESBL- and derepressed AmpC enzyme-producing organisms.38 Various mechanisms are involved in carbapenem resistance.12 In Korea, VIM-2 and IMP-1 type acquired metallo-β-lactamases (MBLs) were reported in these organisms.8,39-41 Certain types of OXA enzymes can hydrolyze carbapenem. Carbapenem-hydrolyzing OXA-23 enzyme was detected in outbreak strains of imipenem-resistant A. baumannii, which involved 36 patients at a university hospital in 2003.42 In Brazilian hospitals, resistance rates of Acinetobacter spp. to carbapenem have reached 12% or higher.43 Thus, more toxic agents, such as polymyxin, have been used, and as a consequence, it was found that 5 out of 100 blood isolates of Acinetobacter spp. were resistant to this drug.
Increasing amikacin resistance in some species of gram-negative bacilli (Table 3) suggest that empirical selection of this aminoglycoside has also became difficult. Fluoroquinolones are frequently used, as they are one of the three major broad-spectrum classes of antimicrobial agents,44 but 56% of Acinetobacter spp. isolates were resistant to this drug.
Compared to the previous report of ampicillin and cotrimoxazole resistance rates (both 34%) of Salmonella enterica serovar Typhymurium DT104,45 the resistance rate to ampicillin was higher, but the rate to cotrimoxazole was much lower. Nontyphoidal Salmonella infections are mostly acquired in communities rather than in hospitals. Therefore, an increase of ampicillin-resistant isolates may suggest prevalence of this resistance in the community. The fluoroquinolone-resistance rate remained very low, but this low rate may not be useful to predict clinical efficacy for the treatment of extra-intestinal Salmonella infections, because low-level quinolone resistance is clinically relevant but not detectable by using fluoroquinolones. A similar ampicillin resistance rate of 47% and β-lactamase production rate of 51% in Haemophilus influenzae isolates in this study suggests that β-lactamase-negative ampicillin-resistant (BNAR) H. influenzae remain rare in Korea, although it has been a prevalent type in Japan.46
In general, resistant bacteria are more prevalent among hospital isolates. However the cefotaxime resistance rate of E. coli (12%) at the commercial laboratory was similar to that in hospitals (14%), suggesting a spread of ESBL-producing strains to the community or to small hospitals. Presence of imipenem-resistant P. aeruginosa and Acinetobacter spp. at the commercial laboratory also suggests a spread of this resistance to small hospitals. The similar fluoroquinolone resistance rates of E. coli at the commercial laboratory (33%) and in hospitals (32%) suggest the presence of fluoroquinolone-resistant E. coli in the community (Table 3). In a Taiwanese surveillance study in 2000, fluoroquinolone resistance is found among isolates from both inpatients and outpatients, not only in medical centers, but also at regional hospitals throughout the country.47
A further increase of cefoxitin-resistant K. pneumoniae was observed in this study (Fig. 2). A previous KONSAR study showed that plasmid-mediated CMY-2 and DHA-1 AmpC-producing K. pneumoniae isolates were prevalent in Korea.8 It is a concern that plasmid-mediated AmpC can confer resistance to imipenem when combined with porin loss.
Acinetobacter spp. showed slight decreased resistance to fluoroquinolone, amikacin, and ceftazidime, but a steady upward trend of resistance to imipenem (Fig. 3). A recent increase in carbapenem usage probably caused these two different trends. In the 2003 KONSAR study,8 many isolates of Acinetobacter spp. showed MDR patterns.
The lower rates of vancomycin resistance in E. faecium, imipenem resistance in P. aeruginosa and Acinetobacter spp., but the similar rate of fluoroquinolone resistance in E. coli at the commercial laboratory in this study, may be due to less use of vancomycin and imipenem, but frequent use of fluoroquinolones in the community or at clinics. Diekema et al.48 analyzed the American Hospital Association annual survey data, and reported a greater prevalence of oxacillin-resistant S. aureus, vancomycin-resistant enterococci, fluoroquinolone-resitant E. coli, and ESBL-producing K. pneumoniae in teaching hospitals than non-teaching hospitals, and in > 199-bed hospitals than smaller hospitals.
In conclusion, oxacillin-resistant staphylococci, expanded-spectrum cephalosporin-resistant K. pneumoniae and fluoroquinolone-resistant E. coli, Acinetobacter spp., and P. aeruginosa were highly prevalent problem organisms in Korea in 2004. Increasing trends were observed for vancomycin-resistant E. faecium, cefoxitin-resistant E. coli and K. pneumoniae, and imipenem-resistant P. aeruginosa and Acinetobacter spp. Some antimicrobial-organisms combinations were also prevalent among the commercial laboratory-tested strains.
OTHER MEMBERS OF KONSAR GROUP
Jae Seok Kim, Hallym University College of Medicine, Seoul; Sunjoo Kim, Gyeongsang National University Hospital, Jinju; Namhee Ryoo, Dong San Medical Center, Keimyong University, Taegu; Seok Hoon Jeong, Kosin University Gospel Hospital, Busan; Mun-Yeun Kim, Dongkook University Pohang Hospital, Pohang; Gyoung-Yim Ha, Dongguk University Kyongju Hospital, Kyongju; Chulhun L. Chang, College of Medicine, Pusan National University, Busan; Ki Hyung Park, Busan Medical Center, Busan; Mi-Na Kim, Ulsan University Asan Medical Center, Seoul; Myungshin Kim, Catholic University of Korea, St. Mary's Hospital, Seoul; Jeong Ho Kim, Yongdong Severance Hospital, Seoul; Joseph Jeong, Ulsan University Hospital, Ulsan; Seok-Il Hong, Korea Cancer Center; Soung Eun Cho, Ewha Womans University Tongdaemun Hospital, Seoul; Jin Ju Kim, Inha University Hospital, Inchon; Hye-Soo Lee, Chonbuk National University Medical College, Chonju; Sook Jin Jang, Chosun University Hospital, Kwangju; Ae Ja Park, Chung Ang University Pil-dong Hospital, Seoul; Young Joo Cha, Chung Ang University Yong San Hospital, Seoul; Dong Hoon Shin, Hallym University School of Medicine, Chunchon Sacred Heart Hospital, Chunchon; Sun Hoe Koo, Chungnam University Hospital, Daejeon; Myung Hee Lee, Korea Veterans Hospital, Seoul; Wonkeun Song, Hallym University College of Medicine, Seoul; Tae Yeal Choi, College of Medicine, Hanyang University, Seoul; Eui-Chong Kim, Seoul National University College of Medicine, Seoul; Jung Oak Kang, College of Medicine, Hanyang University, Kuri; Yeon Joon Park, College of Medicine, Catholic University of Korea, Seoul; Jong Hee Shin, Chonnam University Hospital, Kwangju; Seong Geun Hong, College of Medicine, Pochon CHA University, Seongnam; Young Ah Kim, National Health Insurance Corporation Ilsan Hospital, Goyang; Hee Joo Lee, Kyung Hee University Hospital, Seoul; Dong Hee Cho, Samsung Cheil Hospital; Hwan Sub Lim, Kwandong University Myunggi Hospital, Kyunggi; Miae Lee, Ewha Womans University Mokdong Hospital, Seoul; Hee-Bong Shin, Soonchunhyang University Hospital, Bucheon; Young Ree Kim, Cheju National University Hospital, Cheju; Seung-Ok Lee, Seoul Clinical Laboratories, Seoul; Sung-Hee Lee, Cheju Hanmaeum Hospital, Cheju; and Seong Gyu Lee, Bundang Jesaeng Hospital, Kyunggi, Korea.







 XML Download
XML Download