

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Lymphoblastic lymphomas (LL) represent 1.5% to 4% of all adult non-Hodgkin lymphomas (NHLs).1-4 These high-grade lymphomas are usually composed of precursor T cells, commonly present with mediastinal mass, and have a predilection for young adults.3,4 LLs are aggressive compared to other NHLs, frequently involve the bone marrow and/or central nervous system and are indistinguishable from acute lymphocytic leukemia (ALL) in many respects.3,4
Because of the poor prognosis of LL, many attempts have been made to determine the adequate treatment modality to increase overall survival rates. The current recommended treatment modalities include conventional chemotherapy and peripheral blood stem cell transplantation (PBSCT) after chemotherapy.4 While Lymphomalike treatment regimens such as the Stanford/Northern California Oncology Group (NCOG) protocol had been commonly used for LL to date, ALL-type chemotherapy regimens such as hyper-CVAD (hyperfractionated cyclophosphamide, vincristine, adriamycin, dexamethasone) have been tried for cases with clinical presentation of LL with ALL in several studies.1,3
In Korea, few studies regarding the long-term survival outcome of LL with different treatment modalities have been reported to date. Therefore, we undertook a retrospective study for the patients who received either conventional chemotherapy or PBSCT to analyze the overall survival of adult lymphoblastic lymphoma patients treated with various treatment regimens, and to assess the determinants affecting survival outcomes.
MATERIALS AND METHODS
Patients
We reviewed the medical records of patients with lymphoblastic lymphoma treated in our hospital from June 1996 to June 2005. Among the 31 cases of lymphoblastic lymphoma patients, our analysis excluded six cases, who had not received any kind of treatment or who had not completed at least one cycle of chemotherapy. Twenty-five patients were selected for our study.
The other eligibility criteria common to these patients included a tissue-confirmed diagnosis of lymphoblastic lymphoma, age of 15 years or older, any stage according to the Ann Arbor system, absence of circulating blast cells in the peripheral blood, and normal renal, hepatic and cardiac functions, unless directly attributable to lymphomatous infiltration.
Staging
All patients were staged according to the Ann Arbor system.5 The staging procedure included whole computerized tomographic scans (neck, chest and abdominopelvis), whole body bone scans, positron emission tomography scans, bilateral bone marrow aspiration and biopsy.6 Lactate dehydrogenase (LDH) and albumin levels were measured. Since LDH cutoff values change with the method of measurement over time, we used the LDH index (patient's LDH value/upper LDH cutoff value) to distinguish normal versus increased values.7 Performance status was scored by the Eastern Cooperative Oncology Group (ECOG) scale and allocated into one of several risk groups as described by the International Prognostic Factors Project for NHL.
Treatment and prognosis
The induction regimen for the treatment of lymphoblastic lymphoma was mostly based on adriamycin containing various combination chemotherapy regimens. These included hyper-CVAD (hyperfractionated cyclophosphamide, vincristine, adriamycin, and dexamethasone), m-BACOP (methotrexate, bleomycin, adriamycin, cyclophosphamide, vincristine, and prednisolone), CAVOP (cyclophosphamide, adriamycin, VP-16, vincristine, prednisolone), and CHOP (cyclophosphamide, adriamycin, vincristine, and prednisolone). The Stanford/NCOG protocol was used for treatment in 5 patients. This protocol consisted of a four-phase treatment as follows: (1) induction chemotherapy with cyclophosphamide, doxorubicin, vincristine, prednisolone, and L-asparaginase, (2) CNS prophylaxis with intrathecal methotrexate and whole brain irradiation with 2400 cGy, (3) consolidation chemotherapy with four additional cycles of the drugs used in the induction phase, and (4) maintenance therapy with weekly oral methotrexate and daily 6-mercaptopurine for a total of 12 months of treatment.2 Other chemotherapy regimens used were IMVP-16 (ifosphamide, mesna, methotrexate, etoposide), COPBLAM-V (cyclophosphamide, vincristine, prednisolone, bleomycin, adriamycin, procarbazine) and chemotherapy regimens used in adolescent lymphoblastic lymphoma (prednisolone, vincristine, and asparaginase; prednisolone, vincristine, and adriamycin). Five patients received peripheral blood stem cell transplantation (PBSCT). Of these, four received autologous PBSCT, and one received allogeneic PBSCT. One patient who received the autologous PBSCT experienced a relapse and as such, underwent an allogeneic PBSCT afterwards.
Response criteria
We defined the therapeutic responses according to WHO criteria. Complete remission (CR) was defined as the complete disappearance of all clinical evidence of lymphoma by physical examination and restaging workup, and complete resolution of extramedullary disease. Partial response (PR) was defined as a minimum of a 50% reduction in the sum products of the greatest tumor size and its perpendicular diameter of measurable tumor lesions, persisting for at least 4 weeks. No response (NR) was defined as stable or progressive disease. Relapse was defined as disease recurrence at any site after achieving CR.6
For all patients with or without peripheral blood stem cell transplantation, disease-free survival was defined as the time between confirmed diagnosis and relapse, and overall survival was defined as the time from confirmed diagnosis to death or last follow-up.
Early death was defined as any deaths within twelve months of diagnosis.
Statistical analysis
The disease-free survival (DFS) and overall survival (OS) rates were calculated by Kaplan- Meyer survival plots, and differences between individual survival curves of various prognostic factors were compared by the log-rank test. A p-value < 0.05 was considered to be statistically significant. All calculations were performed using SPSS software, version 12.0 (SPSS Inc, Chicago, IL, USA).
RESULTS
Patient characteristics
The clinical characteristics of the 25 patients are given in Table 1. The median age at presentation was 31.8 years (range, 15 to 72 years). The study population showed the expected male predominance, with 84% of patients having a T-cell immunophenotype and 92% having Ann Arbor stage III or IV disease. According to the IPI risk groupings, 6 patients (24%) had low-risk disease, 13 (52%) had low/intermediate, 5 (20%) had high/intermediate, and 1 (4%) had high-risk disease. The initial performance status according to the ECOG scale was either 0 or 1 in 19 (76%) patients. Eighty percent of the patients presented with multiple lymphadenopathy, and 72% had more than one extranodal involvement. Bone marrow involvement was present in 52% of the patients, but central nervous system involvement was not observed in all study groups.
Treatment
The patients were divided into two groups (conventional chemotherapy versus chemotherapy plus PBSCT) according to the therapeutic modalities they received, as listed in Table 2. Twenty patients (80%) received conventional chemotherapy alone and five (20%) received subsequent PBSCT after chemotherapy. Among the PBSCT group, four patients underwent autologous PBSCT, while one underwent allogeneic PBSCT. One patient who received autologous PBSCT experienced a recurrence 57 months later, and subsequently received allogeneic PBSCT (included in the autologous PBSCT group).
The initial regimens of chemotherapy are listed in Table 3. Eight patients received the hyper-CVAD regimen, five received the Stanford/NCOG regimen, four received the CAVOP regimen, three received the m-BACOP regimen, and one received the CHOP regimen. The remaining patients received a variety of other regimens, including IMVP-16 (ifosphamide, mesna, methotrexate, etoposide), COPBLAM-V (cyclophosphamide, vincristine, prednisolone, bleomycin, adriamycin, procarbazine), and chemotherapy regimens used in adolescent lymphoblastic lymphoma (prednisolone, vincristine, and asparaginase, prednisolone, vincristine, and adriamycin).
Response and outcomes
Of the 25 patients for which treatment could be assessed, 20 responded to induction therapy for an overall response rate of 80% (complete response, 60%; partial response, 20%). The relapse rate was 73.3% (Table 4). With a median follow-up period of 15 months for surviving patients, overall survival was 55.1% at 1 year, 31.5% at 5 years, and 23.6% at 9 years (Fig. 1). The one-year disease-free survival (DFS) rate was 46.7%, and the 7-year DFS was 30.0% (Fig. 2).
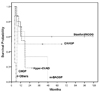
The 5-year overall survival rates for various initial chemotherapy regimens as shown in Fig. 3 were 60% with the Stanford/NCOG regimen, 50% with the CAVOP regimen, 33.3% with the m-BACOP regimen, and 18.2% with the hyper-CVAD regimen Patients treated with other regimens including CHOP and COPBLAM-V expired early in their course.
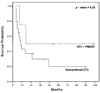
The overall survival rates with conventional chemotherapy and chemotherapy plus PBSCT are depicted in Fig. 4. Overall survival in patients treated with conventional chemotherapy alone was 19.8% at 8 years, whereas patients treated with chemotherapy plus PBSCT showed 50% overall survival at 9 years. The chemotherapy plus PBSCT group showed a higher response rate, but without statistical significance (p = 0.25).
Causes of death
Of twenty-five lymphoblastic lymphoma patients, seventeen patients (68%) expired, seven from infection (sepsis, 57.1%; pneumonia 42.9%), and three as a result of disease progression (Table 5). One patient expired from organ failure, and one from acute myocardial infarction. Of the seventeen expired patients, eleven (64.7%) suffered early deaths, four from infection (sepsis, two patients; pneumonia, two patients), two from disease progression, one from organ failure, and four from unspecified causes.
Prognosis
We compiled information on the prognostic factors (age at presentation, performance status, serum LDH level, Ann Arbor stage, presence of multiple lymphadenopathy, and number of extranodal involvements) associated with the outcomes of these 25 patients to identify independent prognostic factors. In order to select potential prognostic factors, we performed a series of univariate analysis.
The associations between each presenting characteristic and complete response rate, disease-free survival rate, and overall survival rate are listed in Table 6. Old age was a significant prognostic factor associated with a poor overall survival rate (p = 0.01), but was not a significant factor for CR or DFS. Other clinical parameters such as sex, Ann Arbor stage, performance status (ECOG), IPI, immunophenotype, presence of B symptom, multiple lymphadenopathy, extranodal involvement, LDH index, bone marrow involvement, albumin level, and treatment modality were not statistically significant factors for CR, DFS, or OS.
DISCUSSION
Most of the LL patients in this study were young individuals who frequently manifested with stage III or IV (92%), T-cell type (84%), cervical lymphadenopathy (52%), bone marrow involvement (52%), and a mediastinal mass (36%) upon initial diagnosis. These findings were the same as those reported by other studies done in Western as well as Asian countries, demonstrating the similarity in clinical characteristics of lymphoblastic lymphoma among different ethnic groups.3,4
In general, it is recommended that lymphoblastic lymphoma in adults be approached and treated in a manner similar to that for ALL.1 Various adult LL treatment protocols have been presented which are similar to that used in ALL treatment. Both the Stanford/NCOG and hyper-CVAD regimens are well known ALL chemotherapy regimens, but are also used in treating lymphoblastic lymphoma. The complete response (CR) rate and disease-free survival (DFS) rate obtained with the Stanford/NCOG regimen was 80% and 60% respectively, which was comparable to results previously reported in other studies.6,8-10 However, the CR and DFS rates obtained with the hyper-CVAD regimen were 50% and 31.3%, respectively, which were lower than those reported in other studies.3,8 In our study, the overall survival rate was 60% at 9 years with the Stanford/NCOG regimen (Fig. 3) and only 18.2% at 2 years with the hyper-CVAD regimen, showing it to be inferior to those treated with the Standford/NCOG regimen. In contrast, Thomas et al. reported that the estimates for 3-year progressionfree and overall survival for 33 lymphoblastic lymphoma patients treated with the hyper-CVAD regimen were 66% and 70%, respectively.3 Although the hyper-CVAD regimen had become one of the promising chemotherapy regimens in therapy of lymphoblastic lymphoma, it did not show superior results compared to other regimens in our study. The work of Y.C. Chen8 supports our results which suggest that the Stanford/NCOG regimen may be a more effective initial choice of therapy than the hyper-CVAD regimen for lymphoblastic lymphoma.
Peripheral blood stem cell transplantation (PBSCT) is an option for some patients with lymphoblastic lymphoma, particularly those with recurrent or refractory disease.9 Previous studies showed a better survival outcome for a hematopoietic stem cell transplantation group compared with those who received conventional chemotherapy.9,11 In our present work, the overall survival rate was 50% in the PBSCT group and 19.8% in the conventional chemotherapy group after 8 years (Fig. 4). Although the difference in overall survival rate between the chemotherapy plus PBSCT group and the conventional chemotherapy group was statistically insignificant (p = 0.46), a tendency toward a higher survival rate in the PBSCT group was observed, consistent with previous reports.
Several studies have compared the overall survival and relapse rates of autologous and allogeneic transplantation for non-Hodgkin's lymphoma. Levine et al. reported overall survival rates comparable to those in our study for both autologous (56%) and allogeneic transplant recipients (80%), regardless of disease stage, bone marrow involvement, time from diagnosis to transplantation, or other potentially confounding factors.9 In another study by Gouill et al., the analysis of 43 patients with relapsed lymphoblastic lymphoma revealed a higher continuing CR rate in patients with allogeneic BMT (50%) than in patients with autologous PBSCT (14.3%).12 A graft-versus-lymphoma effect may have played a role in the lower relapse rate following allogeneic transplantation.13-15 In our study, one of the patients treated with autologous PBSCT experienced a recurrence 57 months after the procedure, and subsequently received an allogeneic PBSCT. Although the overall survival rate was better in autologous than allogeneic transplant recipients in this study (75% vs. 0% at 15 months, respectively), the number of allogeneic transplant patients were too small to confirm the significance of these results.
The mortality rate was 68% in our study, with infection being the most common cause of deaths (41.2%). Among these cases of infection, 57.1% were from sepsis and 42.9% were from pneumonia. Eleven patients (64.7%) suffered early deaths, with infection (35.4%) being the major cause (sepsis, two patients; pneumonia, two patients).
The mortality rates for the Stanford/NCOG and hyper-CVAD regimen groups were 40% and 62.5%, respectively. Infection as a cause of death was not observed in the Stanford/NCOG group, however, three of the five patients in the hyper-CVAD group died from infection (sepsis, two patients; pneumonia, one patient). It is not known whether the infection source was endogenous or exogenous, and further work is needed to elucidate the causes of infection and to lower mortality rates.
The associations between the various presenting characteristics and complete response rate, disease-free survival rate, and overall survival rate were analyzed. Old age was a significant factor associated with the overall survival rate (p = 0.01), supporting the results of Hahn et al.16 However, old age was not a significant factor for the complete response rate or disease-free survival rate.
Other clinical parameters such as sex, Ann Arbor stage, performance status (ECOG), IPI, immunophenotype, presence of B symptom, multiple lymphadenopathy, extranodal involvement, LDH index, bone marrow involvement, albumin level, and treatment modality were insignificant factors in the complete response rate, disease-free survival rate, and overall survival rate.
In conclusion, the Stanford/NCOG regimen may be an effective initial choice of therapy for lymphoblastic lymphoma patients. Peripheral blood stem cell transplantation should be mandated after achieving complete or partial response with chemotherapy rather than treatment with conventional chemotherapy alone in order to achieve a higher survival outcome. Furthermore, allogeneic transplantation, when an HLA-identical sibling is found, could be an option for young patients in their first CR from a high-risk disease or for relapsing patients in their second CR.







 XML Download
XML Download