

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Vitamin K2 is widely used for the treatment of osteoporosis in Japan. The up-regulation in the expression of bone markers in vivo1 suggests the anabolic action of vitamin K2. Vitamin K2 is known to be a cofactor of γ-carboxylase, which converts the glutamic acid (Glu) residue in osteocalcin molecules to γ-carboxyglutamic acid (Gla) and is, therefore, essential for γ-carboxylation of osteocalcin.2-5 Thus, the role of vitamin K2 in bone formation was thought to be as an essential cofactor for the γ-carboxylation of osteocalcin. However, recent evidence suggests that vitamin K2 also has a transcriptional regulatory function.1 Vitamin K2 is a transcriptional regulator of bone-specific genes that acts through steroid and xenobiotic receptors (SXRs) to favor the expression of osteoblastic markers. Thus, the role of vitamin K2 in the regulation of bone formation may be in the γ-carboxylation of osteocalcin and the mediation of osteoblastic marker expression through the use of SXR, although the exact mechanism remains uncertain. Therefore, the effects of vitamin K2 on bone formation are of interest in the treatment osteoporosis.
However, vitamin K2 has also been reported to inhibit the expression of the osteoclast differentiation factor (ODF)/RANK ligand, tartrate-resistant acid phosphatase activity, and mononuclear cell formation.6 In addition, vitamin K2 has induced osteoclast apoptosis in unfractionated bone cells and isolated osteoclasts on dentine slices, suggesting that the inhibitory effect of vitamin K2 on osteoclastic bone resorption may be exerted via targeting osteoclasts for apoptosis.7 It has also been suggested that the inhibitory effect of vitamin K2 on bone resorption may be independent of the γ-carboxylation system, but related to its side chain.8,9 This line of evidence is substantiated by the anti-resorptive effect of vitamin K2 on bone in vitro.
Clinically, vitamin K2 sustains the lumbar bone mineral density (BMD) and prevents osteoporotic fractures in patients with postmenopausal osteoporosis,10-12 prevents the loss of the lumbar BMD partly by inhibiting the reduction in osteoprotegerin (OPG)13 and reduces the incidence of vertebral fractures in patients with glucocorticoid-induced osteoporosis,14-18 increases the metacarpal BMD in the paralytic upper extremities of patients with cerebrovascular disease or in elderly women with Parkinson's disease,19,20 reduces the incidence of nonvertebral fractures in elderly women with Alzheimer's disease when treated with both vitamin D2 and calcium supplements,21 and sustains the lumbar BMD in patients with liver-dysfunction-induced osteoporosis.22 Furthermore, vitamin K deficiency, which is characterized by an increased circulating level of undercarboxylated osteocalcin and, subsequently, reduced production of γ-carboxylated osteocalcin, may also contribute to the risk of osteoporotic fractures.23-28 Although its effect on BMD may be quite modest, vitamin K2 may have the potential to regulate bone metabolism and reduce the risk of osteoporotic fractures. Thus, vitamin K2 may be useful for treating the various types of osteoporosis by regulating bone formation and resorption. Although it has been recognized that vitamin K2 increases the serum osteocalcin levels, its effect on bone resorption seems to be less certain. To understand the effects of vitamin K2 on bone mass and bone metabolism, we reviewed its effects on the development of osteopenia in rats, the model of osteoporosis.
EFFECTS OF VITAMIN K2 ON THE DEVELOPMENT OF OSTEOPENIA IN RATS
Effects of vitamin K2 in ovariectomized rats
Treatment with vitamin K2 alone
Estrogen deficiency, caused by ovariectomy in rats, resulted in bone loss due to increased bone turnover. Several studies have shown the beneficial effects of vitamin K2 on bone loss in ovariectomized rats. Some studies showed that vitamin K2 prevented early bone loss of the femoral BMD through the inhibition of bone resorption,29 attenuated the increase in osteoclastic bone resorption, 30 maintained the accelerated osteoblastic activity in the femoral metaphysis,30 protected against the loss of trabecular bone mass and its connectivity in the proximal tibial metaphysis (Fig. 1),31 reduced mineralized bone loss in the lumbar vertebra,32 and prevented the decrease in the bone strength of the femoral diaphysis in ovariectomized rats.33 However, other studies, performed by Binkley et al.34 and Otomo et al.,35 showed that vitamin K2 did not reduce ovariectomy-associated elevation of bone turnover and that vitamin K2 did not reduce the distal femoral BMD, bone mass/density, structure, mineral properties (mineral-to-matrix ratio), or the bone strength of the lumbar vertebra and femur. Thus, because of the modest effects of vitamin K2 on the bone mass and/or bone metabolism, its effects on bone loss, formation, and resorption in ovariectomized rats remain controversial. However, vitamin K2 may have the potential to regulate bone metabolism, maintain bone strength or trabecular bone architecture, and at least attenuate bone loss in ovariectomized rats.
Combined treatment with vitamin K2 and vitamin D3
A few studies have demonstrated a preventative effect of this combined treatment on bone loss in ovariectomized rats. Matsunaga et al. (Fig. 2).36 and Hara et al.37 demonstrated that the combined treatment of 1α-hydroxyvitamin D3 and vitamin K2 was more effective for treating bone mass loss in the proximal tibial metaphysis and/or the bone strength of the femoral diaphysis in ovariectomized rats. Although these studies did not clarify the mechanism underlying the beneficial effects of this combined treatment on ovariectomy-induced bone loss, these results illustrated the treatment's additive effect on osteopenia in ovariectomized rats.
Combined treatment with vitamin K2 and bisphosphonates
A few studies have examined the effects of the combined treatment of vitamin K2 and bisphosphonates on osteopenia that was induced by ovariectomy. Ito38 clearly demonstrated that risedronate prevented the deterioration in the connectivity of the trabeculae in the proximal tibial metaphysis in ovariectomized rats, whereas vitamin K2 increased the trabecular thickness. Thus, the combined treatment of risedronate and vitamin K2 had an additive effect in preventing the deterioration of the trabecular bone architecture in ovariectomized rats.
Combined treatment with vitamin K2 and raloxifene
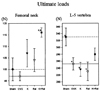
Iwamoto et al.39 demonstrated the skeletal effects of the combined treatment of vitamin K2 and raloxifene in ovariectomized rats. Vitamin K2 alone increased bone formation, whereas raloxifene alone and in combination with vitamin K2 reduced bone turnover. Raloxifene alone, but not vitamin K2 alone, prevented ovariectomy-induced bone loss in the distal femoral metaphysis and proximal tibial metaphysis, as did the vitamin K2 plus raloxifene combination. No significant beneficial effect of either raloxifene or vitamin K2 alone was observed on the femoral neck bone strength; however, vitamin K2 plus raloxifene had greater femoral neck bone strength than the sham-operated controls (Fig. 3). Thus, raloxifene and vitamin K2 had complementary effects on bone resorption and formation activities, respectively, resulting in a significant improvement in the femoral neck bone strength.
Effects of vitamin K2 in orchidectomized rats
Testosterone in males is important for skeletal growth during the period of linear growth and is responsible for the maintenance of skeletal mass at a later stage of life.40-42 Testosterone deficiency, induced by orchidectomy in rats, induced high-turnover cancellous osteopenia43 and cortical osteopenia with cortical porosity and decreased periosteal bone formation.44 A few studies have reported the beneficial effects of vitamin K2 on the cancellous and cortical bone mass in orchidectomized rats. Iwamoto et al.45 showed that orchidectomy in rats induced cancellous and cortical osteopenia by increasing trabecular and endocortical bone turnover in the proximal tibial metaphysis. They also showed that vitamin K2 administration in orchidectomized rats suppressed trabecular bone turnover and endocortical bone resorption, attenuating the development of cancellous and cortical osteopenia. This effect of vitamin K2 on cancellous osteopenia was primarily mediated by its attenuation of the reduction of the trabecular thickness in these rats. These results suggest that vitamin K2 may have the potential to suppress bone resorption or bone turnover, attenuating cancellous and cortical bone loss in orchidectomized rats.
Effects of vitamin K2 in glucocorticoid-treated rats
Glucocorticoid treatment decreased bone formation, which resulted in cortical and cancellous osteopenia in rats.46 A few studies have reported the effects of vitamin K2 on the cancellous and cortical bones in prednisolone-treated rats. Hara et al.47 reported that prednisolone treatment in rats reduced the tibial length, dry weight, bone density, femoral length, bone strength, and calcium content, but vitamin K2 improved these reductions. Hara et al.46 also reported that prednisolone treatment decreased bone formation, resulting in cancellous and cortical osteopenia in the tibia, and that vitamin K2 inhibited the decrease in bone formation, thereby preventing cancellous and cortical osteopenia (Fig. 4 and 5). The results of this study suggest that vitamin K2 may have the potential to prevent bone loss by preventing the decrease in bone formation, as noted in rats treated with glucocorticoid.
Effects of vitamin K2 in sciatic neurectomized rats
Hind-limb immobilization by sciatic neurectomy increased bone resorption and decreased bone formation, resulting in cancellous and cortical osteopenia in the hind-limb of rats.45,48,49 Several studies have reported the effects of vitamin K2 on the cancellous and/or cortical bone mass in sciatic neurectomized rats. Iwasaki et al.48 showed that the cancellous bone mass of the proximal tibial metaphysis was reduced, with a decrease in bone formation and resorption (bone turnover) in sciatic neurectomized rats, and that the administration of vitamin K2 to these rats increased the cancellous bone mass by preventing the reduction in bone formation and further reducing bone resorption. Iwasaki-Ishizuka et al.49 also showed that sciatic neurectomy in rats was associated with a transient increase in bone resorption and a sustained reduction in bone formation, resulting in a reduction in the BMD of the femoral distal metaphysis and diaphysis and also a reduction in the bone strength of the femoral diaphysis, and that vitamin K2 ameliorated these abnormalities. Iwamoto et al.45 showed that sciatic neurectomy in rats increased bone resorption and decreased bone formation in the cancellous bone. They also showed a decrease in periosteal bone formation and an increase in endocortical bone turnover in the cortical bone, resulting in cancellous and cortical osteopenia in the tibia. Vitamin K2 administration in sciatic neurectomized rats suppressed endocortical bone resorption and stimulated bone formation and attenuated the reduction of the trabecular thickness, without any significant effect on the cancellous bone mass, retarding the development of cortical osteopenia in the tibia. These results suggest that vitamin K2 has the potential to suppress bone resorption or bone turnover and/or stimulate bone formation, attenuating cancellous and cortical bone loss in the hind-limb of sciatic neurectomized rats.
Furthermore, Iwasaki-Ishizaka et al.50 demonstrated that vitamin K2 increased the BMD of the distal femoral metaphysis by increasing bone formation and decreasing bone resorption in rats with sciatic neurectomy induced-bone loss. In addition, vitamin K2 increased γ-carboxylated osteocalcin levels and decreased undercarboxylated osteocalcin levels in the serum. These results suggest that vitamin K2 improves osteopenia by improving osteoblast dysfunction and accelerating γ-carboxylation of osteocalcin in sciatic neurectomized osteopenic rats.
Effects of vitamin K2 in tail-suspended rats
Treatment with vitamin K2 alone
Tail-suspension increased bone resorption and decreased bone formation in the cancellous bone and/or decreased bone formation in the cortical bone, resulting in cancellous and cortical osteopenia in the hind-limb of rats.51-53 In particular, suppression of bone formation seemed to play a more important role than the acceleration of bone resorption.54 Iwasaki et al.53 reported that vitamin K2 prevented the acceleration of bone resorption and the reduction in bone formation in the tibia of tail-suspended rats, counteracting the loss of the BMD or cancellous bone mass. Thus, vitamin K2 has the potential to suppress bone resorption and/or stimulate bone formation, attenuating cancellous bone loss in the hind-limb of tail-suspended rats.
Combined treatment with vitamin K2 and bisphosphonates
Iwasaki et al.55 demonstrated that incadronate attenuated cancellous bone loss, by a marked suppression of bone turnover in the proximal tibial metaphysis of tail-suspended rats, and that the combination of incadronate and vitamin K2 led to further attenuation of cancellous bone loss by increasing bone formation, when compared to incadronate alone (Fig. 6). These findings suggest that the concomitant use of vitamin K2 with bisphosphonates ameliorated the suppression of bone formation, which efficiently prevented cancellous bone loss in the hind-limb of tail-suspended rats.
Effects of vitamin K2 in rats with calcium-deficiency
Severe calcium imbalance reduces bone mass in rats. Several studies have reported the beneficial effects of vitamin K2 on osteopenia and calcium balance in calcium-deficient rats. Kato et al.56 reported that a calcium-deficient-diet (low 0.08-0.1% vs. normal 0.8-1.2%) reduced the femoral BMD in rats by 12% and that vitamin K2 reversed calcium-deficiency-induced BMD loss. Iwamoto et al.57 reported that calcium deficiency (low-calcium diet: low 0.1% vs. normal 0.5%) in rats induced hypocalcemia, increased the serum parathyroid hormone (PTH) and 1,25-dihydroxyvitamin D levels, decreased the serum 25-hydroxyvitamin D levels, and stimulated intestinal calcium absorption and renal calcium reabsorption. Calcium deficiency also reduced the cortical bone mass of the tibial diaphysis with decreased periosteal bone gain and an enlarged marrow cavity. Vitamin K2 stimulated renal calcium reabsorption and retarded the increase in the serum PTH levels in calcium-deficient rats. However, since there was no significant change in the serum 1,25-dihydroxyvitamin D levels, vitamin K2 did not appear to have influenced intestinal calcium absorption. Vitamin K2 also retarded cortical bone loss of the tibial diaphysis, primarily by suppressing bone resorption. Robert et al.58 showed that vitamin K deficiency in rats induced hypercalciuria, but did not change the intestinal calcium absorption, and that vitamin K supplementation in vitamin K-deficient rats corrected hypercalciuria.
Kobayashi et al.59 demonstrated that severe calcium/magnesium-deficiency (low-calcium and magnesium diet: low-calcium 0.01% vs. normal 0.5%; low-magnesium 0.003% vs. normal 0.01%) decreased the serum calcium and magnesium levels, as well as the cortical bone mass of the femur, but increased the serum PTH levels and renal calcium excretion. Vitamin K2 attenuated the abnormal decrease in the serum calcium and magnesium levels and the abnormal increase in the serum PTH levels and renal calcium excretion in severe calcium/magnesium-deficient rats.
Kobayashi et al.60 also reported that ovariectomy in rats altered calcium balance, resulting in the decrease in the BMD and the cortical bone mass of the femoral diaphysis. They further noted that vitamin K2 supplementation in ovariectomized rats improved calcium balance and prevented reduction of the cortical bone mass.
These findings suggest that vitamin K2 may have the potential to improve calcium balance, particularly renal calcium reabsorption, and to attenuate cortical bone loss in calcium-deficient rats.
Effects of vitamin K2 in rats with magnesium deficiency
Magnesium deficiency reduces bone strength without affecting the cortical bone mass in rats.61 Kobayashi et al.61 demonstrated that a low-magnesium diet resulted in the reduction of the bone strength of the femoral diaphysis, despite no significant changes in the cortical BMD and cortical thickness. Vitamin K2 also did not affect the cortical BMD or cortical thickness of the femoral diaphysis, but it inhibited a decrease in bone strength.61 These findings suggest that vitamin K2 may be useful in maintaining bone strength in rats with magnesium deficiency.
CONCLUSION
We reviewed the effects of vitamin K2 on the development of osteopenia in rats, the model of osteoporosis. The rats were either ovariectomized, orchidectomized, sciatic neurectomized, tail-suspended, glucocorticoid-treated, or calcium-or magnesium-deficient. It was found that vitamin K2 could regulate bone metabolism in these rats. However, the novelty of the observations is somewhat incremental because most of the pre-clinical animal studies used high-doses of vitamin K2 to test its pharmacological efficacy for bone. Actually, the effects of vitamin K2 on bone mass and bone metabolism seem to be modest. Therefore, molecular changes in bone metabolism need to be investigated to determine the exact mechanisms by which vitamin K2 regulates homeostasis in bones.





 XML Download
XML Download