

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Various pharmacologic agents are known to adversely affect the amplitude and duration of action potentials in the myocardium. Rarely, in patients with implanted permanent pacemakers, pacemaker capture thresholds may be altered by administration of antiarrhythmic agents. Flecainide acetate, a class IC antiarrhythmic agent, has been found to increase the capture threshold by greater than 200%.1-4 The combination of its marked depressant effect on the rate of rise of the action potential, and its relatively small effect on the duration of the action potential, may have a significant effect on myocardial capture threshold.5
We herein report a case of a permanent pacemaker capture failure with an abrupt rise of the capture threshold due to flecainide acetate treatment. The threshold was decreased only after several days of flecainide acetate discontinuation.
CASE REPORT
A 72-year-old male with a medical history of hypertension, diabetes mellitus, and chronic renal failure on scheduled hemodialysis, was referred to our cardiology division for paroxysmal episodes of dyspnea and palpitations. The patient was subsequently diagnosed with paroxysmal atrial flutter and was advised to have sinus rhythm conversion because of distressing symptom during hemodialysis.
One year ago, the patient had a permanent pacemaker (Vitatron Jade 3 SSI model, Medtronic, Minneapolis, MN, USA) implanted due to sick sinus syndrome. Initially, the acute capture threshold was 0.3 V pulse amplitude and 0.4 ms pulse duration. Thus, the pacemaker was programmed in the VVI mode with pacing amplitude of 3.8 V and 0.4 ms pulse duration; it had functioned well until recently.
We treated his atrial flutter with daily administration of oral flecainide acetate (200 mg), and the patient's rhythm converted to sinus within three days. He was discharged, free of symptoms, with a reduced maintenance dose of daily flecainide acetate (100 mg), in order to maintain sinus rhythm.
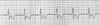
Fifteen days after the flecainide acetate had been started, he was rehospitalized, via the emergency department, due to the development of severe dizziness and episodes of near syncope. The ECG at the time of re-admission revealed complete pacemaker capture failure with a wide QRS idioventricular rhythm of 43/min (Fig. 1). The pacemaker was immediately evaluated, and the ventricular capture threshold was found to be elevated at 5 V at 0.8 ms. There was no evidence of pacemaker lead tip displacement or electrolyte imbalance.
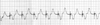
Flecainide acetate was suspected to be the cause of the elevated capture threshold. Therefore, it was immediately stopped, and the capture threshold was adjusted to a maximum level over 5 V at 0.8 ms pulse duration, with a good capture of pacemaker beat (Fig. 2). After discontinuation of flecainide acetate, the capture threshold decreased rapidly. Two days after drug cessation, pacing threshold improved to 2.4 V at 0.8 ms. The patient was discharged with instruction to follow-up at the outpatient clinic.
DISCUSSION
The myocardial threshold to electrical stimulation (capture threshold) is sensitive to a variety of physiologic, pathologic, and pharmacologic changes that affect the heart. Flecainide acetate, a class IC agent, may especially have a profound effect on ventricular capture threshold because of its marked depressant effect on the rate of rise of the action potential and relatively small effect on action potential duration.5 Previous reports have shown that flecainide acetate may cause a greater than 200% or 117% increase in pacing threshold following oral or intravenous administration, respectively.1,2 In our patient, who initially showed an adequate capture threshold and a pacemaker programmed to its maximum output, administration of fifteen days of flecainide acetate led to an abrupt increase in capture threshold from 0.4 V to 5.0 V with subsequent development of pacemaker capture failure. There have been few prior reports which have documented flecainide acetate effect on the moment to moment increase and regression of the ventricular capture threshold. Perez et al.,4 reported these moment to moment changes in capture threshold by analyzing previous records of pacing thresholds. They demonstrated that the threshold increase started immediately following the first dose of medication. The threshold continued to increase even after a stable serum level should have been achieved (by two and half days following initiation of therapy). The temporal course of the ventricular capture threshold provides compelling evidence supporting an adverse effect of flecainide acetate on the ventricular capture threshold. In our experience, we noted that our patient's capture threshold decreased from 5 V to 2.4 V within two days of flecainide cessation.
In retrospect, especially in such a patient with expected unstable pacing threshold, we should have considered the use of a newly developed automatic threshold tracking pacing system. This system verifies ventricular capture beat-by-beat by recognizing the evoked response (ER) following each pacemaker stimulus.7
In addition, it is acknowledged that pacemaker output must be adjusted with a 100% voltage safety margin above the pacing threshold, to avoid ineffective pacing. Schuchert et al.8 reported that low setting of the ventricular pacing output, in pacemaker dependent patients (especially 100%), is not safe in some cases. They suggested that, in patients implanted with low ventricular output programmed pacemakers, an intermittent increment of the pacing threshold should always be ruled out when they have symptoms of ineffective pacing.
Oral flecainide is well absorbed, with peak plasma concentrations occurring two to four hours after dosing. The average elimination half-life is twenty hours after repeated doses. In healthy subjects, approximately 70% of flecainide is metabolized in the liver, and 30% is excreted unchanged in the urine.6 Therefore, dosage should be adjusted in patients with poor renal function. In this case, a number of factors, such as old age and poor renal function, may have enhanced the drug effect.
Since the great majority of implanted permanent pacemaker patients are elderly, and many have similar degrees of cardiac and renal insufficiency,5 we should always consider appropriate dose adjustments of antiarrhythmic drugs. The clinical implication of this case is the fact that flecainide acetate and, possibly, other class IC antiarrhythmic agents, must be used with great caution in patients with implanted pacemakers, particularly if they have impaired renal function.
 XML Download
XML Download