

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
The tension-free vaginal tape (TVT) procedure is simple, minimally invasive, and has become the most popular treatment for stress related urinary incontinence in females.1,2 However, there is growing evidence that this procedure may be associated with serious intraoperative complications, such as vascular injury, obturator nerve injury, and intestinal perforation.2,3 We report an unusual case of intraperitoneal bladder rupture, without concomitant bowel injury, that was unrecognized during a TVT procedure.
CASE REPORT
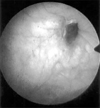
A 35-year-old multiparous woman with no history of surgery or illness presented with a genuine stress related urinary incontinence. She had normal urethral closure pressure and no bladder instability. The patient was selected for TVT placement under spinal anesthesia. Just after insertion of the TVT trocar, the bladder was examined by cystoscopy and there was no sign of perforation. We did not perform an additional cystoscopy after extraction of the trocar. The remainder of the procedure was uneventful. A 16-Fr urethral Foley catheter was used to drain the bladder, and the patient was hospitalized overnight. The next morning, approximately 24 h after surgery, the catheter was removed and she voided without residual urine. Approximately one hour after removing the catheter, she developed acute abdominal pain and a fever. An examination of the suprapubic area revealed diffuse abdominal rebound tenderness without any discharge from the operation site. Vital signs, urinary drainage and laboratory studies showed normal results. Computerized tomography of the abdomen and pelvis demonstrated multiple dilated bowel loops and abnormal fluid collection in the peritoneal space (Fig. 1). A cystogram demonstrated a leakage of contrast media into the peritoneal cavity (Fig. 2). Cystoscopy also revealed a pinhead-sized ulcerative lesion on the right lateral wall, but with no visible perforation into the peritoneal cavity (Fig. 3). Emergency exploratory laparotomy via a lower midline incision revealed general peritonitis, as well as a large intraperitoneal hematoma, with the tape penetrating the pelvic peritoneum without concomitantly causing bowel injury. The right tape penetrated the deep layers of the bladder muscle and mucosa, close to the site of right trocar's passage. The hematoma around the perforated lesion was removed. The retroperitoneal portion of the right tape, just below the bladder rupture site, was cut as low as possible and the tape above the cut area was removed. We did not remove the periurethral and left portions of the tape. The bladder and peritoneum were repaired. The patient recovered with antibiotic management and was discharged one week after laparotomy. The patient's stress-related urinary incontinence remains resolved.
DISCUSSION
Mesh placement using a TVT procedure has unique aspects.2 A curved, five mm needle is placed transvaginally through the periurethral endopelvic fascia, traversing the retropubic space in an upward direction, and is aimed to pierce the anterior abdominal wall close to the pubic symphysis.3 However, the TVT needle may be misdirected at the site of insertion. Bladder perforation caused by a trocar is a common perioperative complication, reported in up to 10% of patients.2,4 Cystoscopy must be performed carefully to detect the misplacement of the tape and penetration of the bladder mucosa. Typical findings of bladder injury are bleeding or erosion of the mucosa.5 However, in this case, we did not observe any perforation during the procedure. Shobeiri et al.4 suggested the possibility of unrecognized bladder lacerations at the initial cystoscopy, and found that three out of six bladder lacerations went unrecognized. Their cadaveric study showed that the trocar might be close to the bladder wall, without necessarily violating the bladder mucosa, at the time of initial cystoscopy. However, occult bladder injury could have been caused after the initial cystoscopy by the rough edge of the plastic covering of the prolene tape advancing during the extraction of the trocar.4 They concluded that such missed occult bladder injury during a TVT procedure was not necessarily caused by a technical failure during the cystoscopy.
Because of the close anatomical proximity, the lower urinary tract structures and viscera are evidently susceptible to surgical injury by the trocar during these procedures.3,4 In the present case, we suspect that the right trocar perforated the peritoneal reflection and the bladder, without concomitant perforation of the bowel or the bladder mucosa. The perforation allowed urine to enter the peritoneal cavity when the patient voided and this led to peritonitis.
The patient had no signs of bladder rupture at the time of surgery. However, because of the subsequent discovery of perforations, we believe that meticulous care should be taken to pass the trocar close to the posterior surface of the symphysis. Additional cystoscopy at the end of the procedure may be helpful to detect such complications, and thus help avoid the need for emergency treatment.


 XML Download
XML Download