

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Coronary anomalies are usually compatible with normal prenatal myocardial development, postnatal myocardial development and postnatal growth and function, and even permit intense athletic activity.1 Congenital anomalous origins of the coronary arteries have been implicated in chest pain, sudden death, cardiomyopathy, syncope, dyspnea, ventricular fibrillation and myocardial infarction.1 The determination of variations in the course and origin of the major coronary arteries is important in coronary surgery and angiography.
Coronary artery anomalies have been discovered as incidental findings during angiography, surgery and autopsy. Coronary anomalies affect about 1% of the general population; this percentage is derived from angiographies performed for suspected obstructive disease.1,2 The reported prevalence of ventricular septal defect (VSD) has varied from 0.3 to 3.3 per 1,000 live births.3 It is a solitary opening, varying in diameter from a few millimeters, but often equaling the diameter of the aortic orifice early in development.4 In adults, VSD constitutes about 10 percent of the congenital cardiac malformations.5 Studies concerning coronary artery anomalies are rather limited in patient with congenital heart defects.6,7 The left anterior descending (LAD) coronary artery arises from the right coronary artery in 4% of the patients with tetralogy of Fallot (TOF).8 The surgical management of TOF may be complicated by anomalies in the course and distribution of coronary arteries.9
CASE REPORT
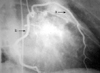
A 38-year-old man was hospitalized for evaluation of angina pectoris. Coronary angiography and left ventriculography were performed through the right femoral artery. In coronary angiography, the right coronary artery was arising from the right sinus of valsalva. The LAD coronary artery arose from the right sinus of valsalva anomalously, just next to the right coronary artery (Fig. 1). The LAD coronary artery was anterior to the right ventricular outflow tract and descended along the anterior interventricular groove. At the beginning, the left main coronary artery arising from the left sinus of valsalva passed between the left auricle and the pulmonary artery. Then, it formed the circumflex branch of the coronary artery. The circumflex coronary artery reached the left atrioventricular groove, and then ran along the posterior part of this groove and terminated to the left of the posterior interventricular groove by giving off branches to the left ventricle and atrium (Fig. 2). In order to determine whether the interventricular opening is congenital or not, it is essential to perform left ventriculography. In the left ventriculogram, a normal chamber and wall motion were observed. We found only a single opening in the membranous portion of the interventricular septum. As a result of this opening, contrast agent was passing from the left ventricle into the right ventricle (Fig. 3).
DISCUSSION
Coronary anomalies may be a part of complex congenital malformations of the heart or may be an isolated defect.10 Congenital anomalies of the coronary arteries may be asymptomatic, or may cause myocardial infarction and sudden death.2 Coronary artery anomalies and VSD are detected by two-dimensional echocardiography, catheterization, surgery, or autopsy.1,3 The anatomic course of the anomalous vessel is found easily through noninvasive imaging techniques, such as MR coronary angiography.2 In our patient, coronary angiography presented an anomaly of the LAD coronary artery and VSD. VSDs are quite common in children but rare in adults because the majority either close spontaneously or are operated on.11 However, it is very rare that the LAD coronary artery originates from the right sinus of valsalva. The anomaly of the LAD coronary artery associated with VSD in our patient is important clinically, since care should be taken in surgical procedures and angiography. In these patients, as angina may be due to compression of the LAD coronary artery between the aorta and pulmonary artery, we are of the opinion that it may be the result of increased pulmonary artery pressure caused by VSD, as in our case.
Presurgical coronary angiography is helpful for documentation of coronary anomalies (in origin, course and distribution) and can help determine the most appropriate surgical approach.12 Congenital coronary artery anomalies were the most common causes (11.8%) of death in US high school and college athletes.13 Yamanaka and Hobbs14 showed that the incidence of anomaly of the LAD coronary artery originating from the right sinus of valsalva was reported to be 0.03% among 126,595 cases. Screening of all subjects with this anomaly is not easy because of its rarity. Therefore, the subjects with this anomaly were found incidentally in angiography or autopsy. Isolated LAD coronary artery originating from the right sinus of valsalva was reported only in seven patients.15-20 Harikrishnan et al.19 reported only one case among 7,400 patients, and Barriales Villa et al.20 two among 13,500 patients.
An LAD coronary artery arising the right coronary artery is usually most commonly associated with TOF.6,21 Massoudy et al.7 investigated 200 postmortem hearts with great arteries transposition. They determined LAD coronary artery anomaly originating from the right coronary artery in 2 out of 78 VSD cases (2.6%). These studies included LAD anomaly with complex cardiac anomalies and could not represent the true incidence of LAD in the general population.6,7 The course of the LAD coronary artery originating from the right sinus valsalva was generally over the right ventricular outflow tract and afterward it reached the anterior interventricular groove.6 In our case, the LAD coronary artery originate from the right sinus of valsalva and crossed anterior to the right ventricular outflow tract and in front of the pulmonary artery, after which it descended to the anterior interventricular groove. In the literature, ours was the first case of LAD anomaly associated with isolated VSD.
In conclusion, we suggest that angiography should be taken for the documentation of anomalies of the LAD coronary artery associated with VSD as it aids in determining the safest surgical procedures.


 XML Download
XML Download