

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
The management of the patients with chronic oral anticoagulation during invasive procedures is problematic. Clinical guidelines and reviews have proposed strategies for perioperative anticoagulation in chronically anticoagulated patients.1-6 However, published recommendations are inconsistent, and not based on well-designed clinical trials. Thus, the relative efficacy and safety of different perioperative management strategies remains unknown.
The risk of postoperative bleeding is related to the adequacy of postoperative hemostasis, the type of procedure, age and the presence of malignancy.4 Conversely, the risk of postoperative thromboembolism is determined by the type of procedure, the clinical consequence of recent thromboembolic event, age and the presence of additional thromboembolic risk factors such as malignancy, antiphospholipid syndrome or hereditary thrombophilic disorders.4
The management of patients with mechanical heart valves is of particular concern to treating physicians. There is also considerable controversy and variation in the recommendations for the prevention of thromboembolism in such patients. Kearon and Hirsh7 suggested that approximately 8 thromboembolic events per 100 patient-years would occur in patients with uncomplicated mechanical valvular prostheses following temporary discontinuation of oral anticoagulants. This risk is much lower than that of patients with a recent episode of deep venous thrombosis (40 cases per hundred patient-years) or arterial thrombosis (15 cases per hundred patient-years). Improvements in prosthetic materials and valve designs have reduced the risk of thromboembolic complications.8 In the most recent version of the guidelines of the American College of Chest Physicians Consensus Conference on Antithrombotic therapy (ACCP), otherwise healthy patients with a bileaflet or tilting disk valve in the aortic position are considered to be at such low risk of thromboembolism that perioperative anticoagulants are deemed unnecessary when warfarin is interrupted for short time periods.3 On the contrary, because patients with a mechanical heart valve in the mitral position are thought to be at high risk, full dose UH or LMWH is recommended.3 Very similar recommendations were previously published by the American College of Cardiology (ACC).2 However, a distinction in the risk of thromboembolic events between mechanical valves in the aortic and mitral positions when oral anticoagulants are temporarily interrupted has not been universally accepted.
In light of the absence of well-designed prospective studies, and the lack of uniformity among clinical guidelines, the hypothesis that "the perioperative anticoagulation management of patients with mechanical heart valves would be heterogeneous" was tested by conducting a survey.
MATERIALS AND METHODS
Korean survey
Between February 2003 to May 2003, a questionnaire with 4 different clinical scenarios (Table 1) was distributed to physicians by e-mail, or direct contact was made by a monitor. Only physicians regularly involved in making recommendations about perioperative anticoagulation from university hospitals were chosen. Two scenarios described the patients with a mechanical heart valve (MHV) in the mitral position, with additional risk factors for a systemic embolism: one undergoing major (scenario 1) and the other minor surgery (scenario 3). Two scenarios described patients with an aortic MHV, one undergoing major (scenario 2) and the other undergoing minor (scenario 4) surgery. Different preoperative and postoperative management options were offered. Treatment options for all scenarios were the same. The questionnaire begins with 5 questions aimed at describing the training and role of the participants involved. In particular, participants were asked about the type of specialties of physicians, the frequency with which they make recommendations about perioperative anticoagulation, whether or not they are affiliated with an Anticoagulation Clinic or Anticoagulation Service, and finally, about whether a guideline exists that addresses the management of patients when oral anticoagulant therapy needs to be interrupted for a procedure exists. All answers were anonymous. The first scenario described "a 70-year-old woman, with a mechanical mitral valve, chronic atrial fibrillation, and a previous stroke two years earlier, who was to undergo an elective (open) subtotal colectomy for resection of an adenocarcinoma of the colon". The second scenario described "a 65-year-old man, with a mechanical bileaflet aortic valve, who was to undergo an elective (open) subtotal colectomy for resection of an adenocarcinoma of the colon, but had no other medical problems". The third scenario described "a 75-year-old man, with a mechanical mitral valve, a previous stroke 3 years earlier and chronic atrial fibrillation, who was to undergo an elective bilateral inguinal hernia repair". The fourth scenario described "a 48-year-old woman, with a mechanical bileaflet aortic valve, who was to undergo an elective bilateral inguinal hernia repair but had no other medical problems". For each of the 4 scenarios presented, 4 options were proposed for the preoperative management and 5 or the postoperative management of the patients. The anticoagulation options are presented in Table 2.
RESULTS
Of the 90 questionnaires distributed, 52 (57.8%) were returned. Of the 52 physicians responding to the questionnaire, cardiologists were the best represented (n=21, 41.2%), followed by hematologists (n=13, 25%), cardiac or vascular surgeons (n=12, 23.5%) and internists (n=3, 5.9%). Forty-one of the participants returning the questionnaire (78.5%) were affiliated with an Anticoagulation Clinic or an Anticoagulation Service. Of these, 35 (83.3%) reported that they used local guidelines to decide upon the perioperative management strategy when oral anticoagulant therapy was temporarily discontinued.
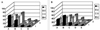
The results from the survey are shown in Fig. 1. The first scenario described a patient with a high thromboembolic risk undergoing a surgical procedure considered high risk for both thrombotic and hemorrhagic complications. Admission to hospital for full-dose IV UH was the most frequently selected anticoagulation option for preoperative anticoagulation (n=30, 58.8%), followed by "outpatient full-dose subcutaneous (SC) UH or LMWH" (n=17, 33.3%) and "nothing else other than holding warfarin" (n=3, 5.9%). One physician selected "low-dose subcutaneous UH/LMWH". For the postoperative management, "full-dose SC UH or LMWH" was the most frequently selected anticoagulation option (n=27, 52.9%), followed by "full-dose intravenous UH" (n=17, 33.3%). Six physicians (11.8%) selected "low-dose SC UH or LMWH" and one "nothing else other than restarting warfarin" after the operation. No physician selected an alternative anticoagulation strategy.
The second scenario described a patient at low risk of thromboembolic events, according to the last ACCP guidelines,3 undergoing a surgical procedure considered high risk for both thrombotic and hemorrhagic complications. For the preoperative management, admission of intravenous full-dose UH (n=21, 42%) and full-dose LMWH (n=21, 42%) were the two most frequently selected anticoagulation options, followed by "nothing else other than holding warfarin" (n=5, 10%). Three physicians selected outpatient low-dose SC UH and one did not respond. For the postoperative management, both full-dose SC and low-dose UH or LMWH were the two most frequently selected anticoagulation options (n=17, 34%), followed by full-dose intravenous UH(n=14, 28%). Two physicians (4%) selected nothing else other than restarting warfarin after the operation and one did not respond.
The third scenario described a man at high risk for thromboembolic complications undergoing a low risk surgical procedure. For the preoperative management, 22 participants (44%) selected intravenous full-dose UH (n=22, 44%), followed by full-dose LMWH (n=21, 42%) and nothing else other than holding warfarin (n=5, 10%); two respondents chose low-dose SC UH and one did not respond. For the postoperative management, hospitalization for intravenous full-dose UH (n=16, 32%) and full-dose SC or LMWH (n=16, 32%) and low-dose SC or LMWH (n=15, 30%) were the most frequently selected anticoagulation options. Three physicians (6%) selected nothing else other than re-starting warfarin postoperatively.
The fourth scenario described a woman at low embolic risk, according to the ACCP guidelines, undergoing a low risk surgical procedure. For the preoperative management, outpatient full-dose LMWH (n=24, 48%) was the most frequently selected anticoagulation option, followed by administered full dose subcutaneous UH (n=17, 34%) and nothing else other than holding warfarin (n=6, 12%). Three physicians selected outpatient low-dose subcutaneous UH and one did not respond.
For the postoperative management, 17 participants (34%) selected low-dose subcutaneous UH or LMWH, followed by full-dose subcutaneous UH or LMWH (n=14, 28%), and full-dose intravenous UH (n=12, 24%). Seven physicians (14%) indicated they would simply reintroduce warfarin without administering any additional antithrombotic treatment.
The preoperative and postoperative choices for each scenario were compared with the results from a 1997 distribution of this survey to Canadian providers (Fig. 2). Compared to the Canadian physicians, the Korean physicians chose LMWH more frequently in all four scenarios.
DISCUSSION
In this survey, the physician preferences for the perioperative anticoagulation management of patients with mechanical heart valves were investigated. Three main issues were raised by our results. (1) Guidelines2,3 suggesting patients with a mechanical aortic valve do not need any perioperative anticoagulation are not universally accepted. (2) There is no clear consensus on the peri-operative management of patients receiving oral anticoagulant treatment. (3) LMWH has been increasingly accepted as a perioperative anticoagulant for patients whose oral anticoagulant therapy must be interrupted.
In recent years, long-term follow up studies have shown that patients with a bileaflet valve (St. Jude Medical or Carbomedics) or tilting disk valve (Medtronic-Hall) in the aortic position, and who were in a normal sinus rhythm and have a left atrium of normal size, were at low risk of a systemic embolism,10-12 so a lower INR range, between 2.0 and 3.0, is now recommended.13 However, whether this finding implies a lower risk of a systemic embolism during the short intervals when warfarin has been discontinued needs to be confirmed by well-designed prospective studies.
The answers to our questionnaire revealed a substantial variability in the choice between full and low dose UH or LMWH in both the high and low risk situations. Intravenous full dose heparin was the most frequently selected anticoagulant option, especially in patients with a very high thrombotic risk: 58.8% of participants prescribed full dose UH in the preoperative phase for patients with a mitral valve prosthesis and history of stroke. Conversely, the responses for patients with lower thrombotic risk were less uniform. In the preoperative phase, for a patient with a mechanical aortic valve and no concomitant thrombotic risk factor, 34% of participants prescribed full-dose UH, whereas 48% prescribed LMWH and 18% no or lower dose heparin until restarting warfarin postoperatively. For all four scenarios, the rate of participants selecting full-dose intravenous UH decreased from the preoperative to the postoperative phases, from 58.8 to 33.3% in the first scenario, 42 to 28% in the second, 44 to 32% in the third, and from 34 to 24% in the forth. Apparently, when warfarin is reintroduced many physicians feel comfortable in administering subcutaneous LMWH/UH instead of intravenous full-dose UH until the INR reaches a therapeutic range. It is possible they consider this strategy to have a lower bleeding risk than IV UH during the postoperative period.
Although full-dose intravenous UH is still indicated by clinical guidelines,2,3,5 LMWH is gradually taking the place of UH in many clinical settings. This acceptance is justified by the results obtained in many trials comparing UH and LMWH for the treatment of venous thromboembolism and acute coronary syndromes.14 Although, evidence suggests that LMWH has comparable clinical efficacy and better cost-effectiveness than intravenous UH as a perioperative anticoagulant.15-17 However, because the published experience in this area consists of small uncontrolled cohort studies,18-24 some physicians are still reluctant to use LMWH, despite its advantages over unfractionated intravenous UH as a perioperative anticoagulant.
The results of our survey are likely to be relevant. Although, the answers were received from only a small number of physicians, with most regularly involved in making recommendations about perioperative anticoagulation in their hospitals, and many involved directly in the local production of clinical guidelines for this purpose. Thus, the results of our survey probably accurately represent the Korean practice patterns.
In conclusion, there is still uncertainty on the optimal perioperative management of chronic anticoagulation patients having mechanical heart valves. Prospective clinical trials will be required to better guide clinicians in their choice of the intensity and type of perioperative antithrombotic strategies according to the thrombotic risk.



 XML Download
XML Download