

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
The infusion rate of a drug is based frequently on body weight. There is a progressive decline in lean body mass and, particularly, in muscle with aging, and blood volume and extracellular fluid also diminish with age. Hence, the central volume of distribution for highly polar compounds should be smaller, and the dosage based on body weight will result in a higher initial plasma concentrations than for the young adult.1 The decreased total body water and liver mass, which normally accompany aging, are likely explanations for the prolonged duration of action for the neuromuscular blockade compounds in the elderly.2,3 Various pharmacokinetic factors may also be involved in the delivery of a drug.
Rocuronium bromide is structural analogue (2-morpholino, 3-hydroxy, 16N-allylpyrrolidino derivative) of vecuronium with a neuromuscular blocking potency 6-7 times less that of vecuronium. This lack of potency is thought to be an important factor in determining the rapid onset of neuromuscular block.4,5 Rocuronium is a nondepolarizing muscle relaxant with an intermediate duration of action and insignificant accumulation, and it is well suited for continuous infusion.6-8 Rocuronium is eliminated primarily by the liver and to a slight degree by the kidneys. Because rocuronium does not have active metabolites,9 it may be a better choice than vecuronium for prolonged infusion.
The infusion rate of rocuronium for an adequate surgical operation was suggested to be 6.1 ± 2.0 µg/kg/min10 and 8.4 ± 1.6 µg/kg/min8 for adult and pediatric patients, respectively, during sevoflurane anesthesia, while there has been no report yet on the optional dosage for elderly patients.
The aim of this study was to determine the infusion rate of rocuronium necessary to maintain a stable and suitable level of neuromuscular blockade for surgery in young adults and the elderly patients. We also evaluated different anthropometric variables such as body weight, ratio of weight to body surface area (BSA), sum of subscapularis and suprailiac skin folds, body mass index (BMI) and percentage of ideal body weight (%IBW) as indices for the optimization of rocuronium administration to each individual patient.
MATERIALS AND METHODS
After obtaining approval from the Local Ethics Committee and written informed consent, 60 patients (ASA physical status I or II) who were scheduled for elective orthopedic surgery under general anesthesia were assigned into two groups: 1) young adult patients aged 20 to 50 years (control group, n = 30); 2) elderly patients aged over 65 years (elderly group, n = 30). Exclusion criteria were body weight more or less than 20% of the ideal body weight, expected difficult intubation, pre-existing hepatic, renal and neuromuscular disease, allergic diathesis, pregnancy or breast-feeding and preoperative medication known to interact with non-depolarizing neuromuscular blocking agents.
Anthropometric variables such as height, weight, and subscapularis and suprailiac skin folds were measured before the induction of anesthesia. BSA was estimated using the formula of Du Bois and Du Bois11 (0.007184×height [cm]0.725×weight [kg]0.425) and BMI calculated as total body weight divided by the squared height.12 Calculation of the ideal body weight (IBW) was based on the formula of Devine13,14 {50 kg + 2.3×(height [inch]-60) for man and 45.5 kg + 2.3×(height [inch]-60) for woman}.
Patients were premedicated with glycopyrrolate 0.2 mg and midazolam 2.0 mg that was given intramuscularly 30 min before surgery. Each patient was given a standard general anesthetic consisting of fentanyl, thiopental sodium, 50% nitrous oxide and 3% sevoflurane in oxygen. The neuromuscular blockade was monitored using an accelerograph TOF-Watch® (Organon, Teknica B.V., Boxtel, the Netherlands). The patient's arm used for neuromuscular monitoring was fixed to an arm board. The ulnar nerve was stimulated transcutaneously at the wrist via reference electrodes. After calibration, supramaximal stimuli of 0.2 ms duration in a single twitch mode at 1 Hz were used until the end of the study. The software that the computer used to record the responses was TOF-Watch®. Another anesthesiologist behind a screen, who positively could not see the patient, observed only the TOF-Watch® and then he or she adjusted the infusion rate of rocuronium. Non-invasive blood pressure was measured on an arm, and the arm was not used for the evaluation of neuromuscular transmission. Fluids were given via an intravenous cannula inserted proximal to the area of nerve stimulation.
An ED95 dosage (0.3 mg/kg) of rocuronium was administered via a forearm vein and then tracheal intubation was performed when the maximal depression of the twitch response was reached. When the height of the single twitch recovered up to 15% of the control twitch recorded before induction of the neuromuscular block, the continuous infusion of rocuronium was initiated. The continuous infusion rate was determined when the single twitch response was maintained at 10 ± 5% for more than 10 minutes and forty minutes after 1.5-2.0% sevoflurane was reached.10 Mechanical ventilation was adjusted to maintain the end-tidal carbon dioxide partial pressure between 30 and 35 mmHg. Body temperature was monitored continuously in the upper esophagus and at the thenar eminence of the same arm used for neuromuscular monitoring. Core temperature and skin temperature were maintained at greater than 36.0℃ and 32.0℃, respectively.
Data were expressed as means ± standard deviation. The anthropometric variables and infusion rates of the two groups were compared by t-test and a p-value < 0.05 was considered statistically significant. The linear regression analysis was used to test the relations between the anthropometric variables and the infusion rate. To determine the correlation, individual values of each anthropometric parameter were also plotted against the infusion rate provided. Data were analyzed using SPSS for Windows software (SPSS 11.0, Chicago, IL, USA).
RESULTS
There were no significant differences between the young adult and the elderly patients for the anthropometric variables like height, weight, BSA, BMI, %IBW, ratio of body weight to BSA and the sum of subscapularis and suprailiac skin folds. The infusion rate of rocuronium (2.9 ± 1.0 µg/kg/min) in elderly patients was significantly less than that of young adults (4.2 ± 1.6 µg/kg/min) (p < 0.05, Table 1).
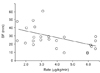
The infusion rate of rocuronium in young adults correlated with the sum of subscapularis and suprailiac skin folds (r2 = 0.23, p = 0.007, Fig. 1). However, the elderly did not show any correlation with the anthropometric variables.
DISCUSSION
The present study demonstrated that the infusion rate of rocuronium in the elderly under sevoflurane anesthesia was about 69% less compared to that in the young adults.
This is consistent with earlier findings for vecuronium in other study. The vecuronium infusion rate was 70% less in the elderly than that in the young adults.15 The most reasonable explanation for the decrease of the infusion rate in the elderly would be a decrease in drug elimination capacity noted with aging. In addition, pharmacokinetic changes in the elderly such as reduction in the total body water and liver mass may result in a prolonged effect of rocuronium.3,16
The continuous infusion of a neuromuscular blocking agent stabilizes the blood concentration of the drug maintains the degree of neuromuscular relaxation constant.17 When the infusion dosage is adjusted to the appropriate individualized demand for each patient, it is possible to avoid excessive neuromuscular relaxation by reducing the total drug requirement. A more rapid recovery from the neuromuscular relaxation by using a proper antagonist within a short time after the infusion termination is a decided advantage.18 However, neuromuscular monitoring is a necessity because interindividual differences do exist.19 Infusion rates based on weight may provide a relatively excessive dosage to the elderly because of their pharmacokinetic differences. If other anthropometric besides body weight can predict infusion rate, they can be clinically useful indices.
As for the initial infusion rate, the infusion rate of rocuronium in elderly patients should be reduced since the infusion rate needed to produce adequate surgical relaxation in the elderly was significantly less than that used in the young adult. The infusion rate in the elderly must be individualized for the special requirement of each patient, and this means starting at a lower infusion rate for the elderly.
It has been suggested in several studies that the volatile anesthetics elicit strengthening of the neuromuscular relaxation.8,10,17,20-22 In particular, when compared with the intravenous anesthetic, propofol, the use of a volatile anesthetic decreases the infusion rate of rocuronium by 40%.10 The infusion rate of rocuronium in this study was lower than those reported in the previous studies4,7,8,17,21,22 presumably due to the neuromuscular blocking effect of sevoflurane. Although the exact mechanism of neuromuscular relaxation by a volatile anesthetic has not been elucidated, an interaction between a volatile anesthetic and a neuromuscular blocking agent is known to enhance the inhibition of the muscular contraction and to move a neuromuscular blocking agent dosage-response curve to the left (the decrease of ED50, ED95).17
In young adults, the sum of subscapularis and suprailiac skin folds is the best predictor for the infusion rate of rocuronium. Therefore, the infusion rate of rocuronium should logically be based on the sum of subscapularis and suprailiac skin folds. Using the sum of subscapularis and suprailiac skin folds to determine the infusion rate is a safe method even in the obese patients because the prolongation of the muscle relaxant effect is avoided since an overdose is prevented.23 The elderly did not show any correlation with standard anthropometric variables.
The skin fold measurement predicts the body density and is used to calculate the body mass percentage. The skin folds can be measured at several regions such as thigh, abdomen, triceps, biceps, chest, subscapularis and suprailiac regions. Among these, only the subscapularis and suprailiac skin folds were measured in our study because it was not necessary to measure the skin folds on several regions, since a significant result was obtained from previous studies for vecuronium by applying the sum of subscapularis and suprailiac skin folds.24
The continuous infusion rate of rocuronium based on the 10% twitch height with accelerography under sevoflurane anesthesia for the elderly over 65 years old was 2.9 ± 1.0 µg/kg/min. Unlike young adults, there were no significant anthropometric predictors to determine the infusion rate of rocuronium in the elderly. From these results it was concluded that the infusion rate of rocuronium in the elderly should be reduced and an adequate infusion rate has to be individualized by the use of a neuromuscular monitor.

 XML Download
XML Download