

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Behçet's disease (BD) is a polymorphic and systemic disease that affects multiple organs with a variety of symptoms. It has been speculated that viral, and streptococcal infections, environmental factors, racial and familial tendency, and autoimmune mechanisms might play a role. The underlying pathology in all these lesions is nonspecific vasculitis of small and large vessels.1 Severe vasculitis induces necrosis, which can result in fistula formation between the neighboring tissues. Patients in whom medical therapy has been unsuccessful, or those who have extensive disease or complications, should be considered for surgery. In the present study, eleven patients with a fistula combined with BD, including clinical finding, treatment, and prognosis, are reviewed.
MATERIALS AND METHODS
The medical records and radiological studies of the patients presenting at the Behçet's Disease Specialty Clinic of our institutions, between 1990 and 2004, and who fulfilled the criteria of both the International Study Group for Behçet's Disease2 and the revised criteria of the Behçet's Disease Research Committee of Japan,3 were retrospectively reviewed, revealing eleven patients with a combined fistula. The mean age of the patients at the time of BD diagnosis was 30.2 years, ranging from 18 to 39 years. The interval between the initial diagnosis and that of the fistula was, on an average, 4.9 years. The clinical characteristic of the BD patients with a fistula are listed in Table 1.
RESULTS
Enterocutaneous and enteroenteric fistula
Total 6 patients (3 cases with enterocutaneous fistulae and 3 cases with combined enterocutnaeous and enteroenteric fistulae) were enrolled in the study. All cases developed after previous surgical manipulations with or without relation to gastrointestinal BD, and durations were variable (7 months to 2 years) between operation and fistula formation. Two cases showed no recurrence, but in 4 cases multiple recurrences were observed in both fistula types. Although mild lesions were medically observed and healed spontaneously in most conditions, there were several situations needed surgical repair thereafter.
Rectovaginal fistula
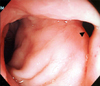
Two patients were reported with rectovaginal fistula. One developed five months after transanal endoscopic microsurgery (Fig. 1) and the other developed after hemicolectomy for obstruction. Although appropriate surgical repairs were performed in each conditions, recurrences were not controlled well.
Urethrocutaneous fistula
Single case was enrolled with multiple ectopic urethral meatuses around the glans penis and penile shaft, which were healed with dressings without the need for surgical interventions (Fig. 2). The lesion had recurred several times during the last 6 years, but healed the same way each time.
Urethrovaginal fistula
In a patient an urethrovaginal fistula was observed after an ureterorenoscopy for a ureteral stone. Although multiple primary repairs were performed, but each times fistulae recurred soon thereafter. Finally complete bladder neck closure and a suprapubic cystostomy were performed.
Aortoduodenal fistula
Four years following a graft interposition of an aortic aneurysm, an aortoduodenal fistula was detected in a patient, which was thought to be a primary lesion of sudden septicemia and gastrointestinal bleeding. Re-interposition of the aortic graft and a segmental resection of the duodenum were performed, but the patient expired 48 hours postoperatively.
DISCUSSION
A fistula is an abnormal, narrow channel or tract connecting between neighboring tissues, which can develop in the presence of inflammation and infection. It may or may not be associated with an abscess, but as with an abscess, certain illnesses, such as BD and Crohn's disease, can cause fistulae to develop.4
In the present study, fistulae formations combined with BD were observed in eleven cases, including enterocutaneous, enteroenteric, rectovaginal, urethrocutaneous, urethrovaginal and aortoduodenal fistulae. Other types of fistulae have been reported in the lieterature, such as vesicovaginal,5 broncho-pulmonary arterial,6 aortoatrial,7 tracheoesophageal,8 arteriovenous9 and arterioportal fistulae.10
The exact mechanism of fistula formation in BD is unclear. In general, fistula formation is associated with poor nutrition, infection, and long term steroid use.11 In nine of our cases (case 1, 2, 3, 4, 5, 6, 8, 10, and 11), the fistulae developed after surgical processes. The fistulae were assumed to have developed due to the severe vasculitis in BD that results in an ulcer and necrosis, along with a pathergy reaction due to surgical trauma. However, the long term use of systemic corticosteroid might also have contributed to the fistulae formation.
In the present study, enterocutaneous and enteroenteric fistulae were the most common. BD is well known to often be accompanied by gastrointestinal involvement.12 The predilection sites are the terminal ileum and ileocecal area, but ulcers can develop along the entire colon. The ulcers are sometimes transmural, leading to perforations or fistula formation, or both.13 In general, an enterocutaneous fistula occurs after severe ulceration, correction operation, or even en appendectomy. Furthermore, most of these recurrent ulcers were noted at or near the anastomotic site.
A rectovaginal fistula combined with BD is very rare, with only five cases having been reported.14 Most patients included in these cases had severe vulval and anorectal ulcers.
Urinary tract involvement in BD can include glomerulonephritis, amyloidosis, cystitis, epididymitis,15 orchitis, and ulcerations affecting the scrotum, penis, vulva and vagina. Rare cases of urethrovaginal and vesicovaginal fistulae have been reported,16 but an urethrocutaneous fistula remains to be reported.
Fistulae seem to be an operative challenge for the surgeon, as they tend to be associated with significant scarring and insufficient surrounding tissues to allow for a tension-free closure. For this reason, interposition of the tissue for good vascular supply is necessary to facilitate healing. There have been case reports illustrating the advantage of interposing healthy tissue, like omentum or a dermofat graft, between the layers.16
Vascular death is most often caused by aneurysm formation and the inflammation occurring in the media and adventitia of large arterial lesions is characteristic of vasculo-BD. It has been postulated that active arteritis occurs initially, followed by destruction of the media and fibrosis in the affected arteries. An aortoenteric fistula is an uncommon, but life-threatening cause of gastrointestinal blood loss, which is often rapid, leading to death by exsanguinations.17 Our patient expired in the immediate postoperative period.
Most fistulae are corrected by operation, but anti-TNFα antibody treatment has recently challenged.18 The fistula has a tendency to recur, and reoperation of the fistula in BD seems to be the cause of the vicious cycle of frequent recurrences.
BD is accompanied by various types of fistula formation. The fistula formations in BD are closely related to the underlying vasculitis with various inflammatory cytokines as the pathogenesis of BD and the mucocutaneous hyperreactivity (Pathergy reaction) to trauma which is quite unique phenomena.
In the endemic area of BD, we must consider about the possibility of postoperative fistula formation in the BD patients and the differential diagnosis of BD when wound healing is impaired or a fistula formed after surgery.

 XML Download
XML Download