

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
According to statistics from the 1999 Ministry of Health & Welfare of South Korea, pancreatic cancer ranked 8th and 10th among cancers in incidence in men and women, respectively, and the rate is increasing.1 Smoking, high-calorie diets, certain chemical exposures, chronic pancreatitis, cystic fibrosis, and diabetes are known to induce pancreatic cancer; however, no exact cause has been identified.2
Even after curative resection, pancreatic cancer has a poor prognosis due to low resection rates and late diagnosis. Only 15-20% of cases undergo resection, and 5-year survival is approximately 20%.3,4 In addition, adjuvant therapies have not yet been standardized.
Several oncogenes and tumor suppressor genes have been shown to be associated with cancer pathogenesis, and molecular-based treatment approaches are being attempted for various cancers, including pancreatic cancer.5 Major genes related to pancreatic cancer include K-ras, p53, p16, and DPC4.6-8
The p16 gene, also called MST1 or CDKN2, is a tumor suppressor gene located on chromosome 9p21. By binding to cyclin-dependent kinase 4, the p16 protein inhibits phosphorylation of various growth and regulation factors which control proliferation in the G1 period of the cell cycle. When p16 genes are mutated, cyclin-dependent kinase 4 activation is increased and hyperphosphorylation of Rb protein occurs, leading to accentuated progression of the cell cycle from G1 to S and to cell proliferation.
P53 is located on chromosome 17p; it is a cell cycle checkpoint and induces apoptosis. If p53 gene functions are inactivated, control of cell proliferation and induction of cell apoptosis, two major regulations in cell growth, are lost.
Ongoing studies evaluating the association between genes and the clinical or biological properties of pancreatic cancer have shown various results. In addition, current studies aim to identify the carcinogenic phase, in which various tumor suppressor genes and oncogenes are converted from normal cells to cancer cells.
The aims of this study were to detect p16 protein expression loss and p53 protein overexpression in pancreatic cancer using immunohistochemical staining, to analyze the clinicopathologic characteristics and their relation to survival rate and to determine the clinical significance of p16 and p53 genes and their interaction.
MATERIALS AND METHODS
Patients diagnosed with pancreatic ductal adenocarcinoma who underwent curative resection in the Department of Surgery, Yonsei University, College of Medicine between March 1990 and April 1999 were eligible for the study. Ultimately, 44 subjects with appropriate paraffin-embedded tissue samples and follow-up data were selected.
Examination of clinical records
We retrospectively examined medical and pathological records to identify clinical and histopathological characteristics of subjects.
Immunohistochemical examination
p16 protein immunohistochemical staining
The 5 µm serial sections of each block were adhered to poly-L-lysine covered slides, and heated at 50℃ for 1 hour. After paraffin elimination with Xylene and a staged ethyl alcohol dehydration, sections were placed in methanol (300 ml) and hydrogen peroxide (10 mL) for 20 minutes in order to saturate endogenous peroxidase. After washing in water, sections were placed in citrate buffer solution and heated for 20 minutes. After cooling, samples were processed with TRIS buffer solution for 10 minutes. Sections were then incubated for 12 hours with p16 antibody (Santa Cruz Biotechnology, Inc, Santa Cruz, CA, USA), diluted at a 1:100 ratio. After washing with TRIS buffer solution, sections were stained using the Universal LSAB peroxidase II kit (Dako, Carpenteria, CA, USA) and developed by diaminobenzidine.
p53 Immunohistochemical staining
A 1:200 dilution ratio of p53 antibody (Novocastra, Benton, NC, UK) was used for p53 immunohistochemical staining. The remaining procedure was identical to the p16 protein immunohistochemical staining process.
Immunohistochemical staining results
Positivity for p16 and p53 immunohistochemical staining was microscopically determined by identification of dark brown-stained nuclei. The sample was considered p16 or p53 protein positive in cases that had 5% or greater positive cells from 1,000 cells under high magnifying power (×400).
RESULTS
Of the 44 subjects, there were 30 men and 14 women; the average age was 57 (range: 39 to 75) years. Thirty-eight tumors were at the head of the pancreas (86.4%) and 6 were in the body or tail (13.6%); more were located at the head, as tumors in that location have greater curative resection possibility than those in the body or tail.
Cell types included 41 (93.2%) cases of ductal adenocarcinoma and 3 (6.8%) cases of mucinous ductal adenocarcinoma. Of the ductal adenocarcinoma cases, 6 (14.6%) were well-differentiated, 21 (51.2%) were moderately-differentiated, and 14 (34.1%) were poorly-differentiated. Size and depth of tumor invasion classified by the American Joint Committee on Cancer (AJCC) criteria of T1, T2, T3, and T4 class were 3 (6.8%), 2 (4.5%), 35 (79.6%), and 4 (9.1%) cases, respectively; T3 was the most common class in our study population. Lymph node metastasis was evident in 19 (43.2%) cases. According to AJCC staging, the number of patients with stage I, II, III and IV cancer were 4 (9.1%), 18 (40.9%), 18 (40.9%), and 4 (9.1%), respectively (Table 1).
By immunohistochemical staining, there were 20 (45.5%) cases with negative p16 protein expression and 14 (31.8%) cases with positive p53 protein expression (Fig. 1, 2).
Negative p16 protein expression occurred in 13 (43.3%) of 30 men and 7 (50.0%) of 14 women, indicating no difference between the sexes. Negative p16 protein expression was not significantly different among histologic differentiation or T-staging. Negative expression occurred in 3 (50.0%) well-differentiated, 11 (52.4%) moderately-differentiated, and 5 (35.7%) poorly-differentiated tumors, and in 2 (75.0%), 1 (50.0%), 14 (40.0%), and 3 (75%) cases in T1, T2, T3, and T4 classes, respectively. There was a statistically significant difference of negative p16 protein expression between cases with and without lymphatic metastasis, 8 (32.0%) and 12 (63.2%), respectively (p=0.040). There was also a statistically significant difference between stage I and II vs. stage III and IV cases, 6 (27.3%) and 14 (63.6%), respectively (p=0.015) (Table 2).
Overexpression of p53 protein was demonstrated in 11 (36.7%) men and 3 (21.4%) women, showing no difference among sex. With regards to histologic differentiation, overexpression was present in 0 (0.0%), 7 (33.3%), and 7 (50.0%) cases with well-, moderately, and poorly differentiated tumors, respectively; thus indicating that frequency of p53 overexpression is correlated to extent of differentiation (p=0.038). There was no significant difference between expression of p53 protein and tumor size, depth of invasion, lymph node metastasis, or pathologic staging (Table 3).
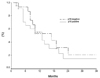
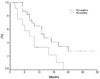
The overall disease-free survival rate of patients with and without p16 protein expression was 18 and 21 months, respectively, showing no statistically significant difference (Fig. 3). However, disease-free survival of patients with and without p53 overexpression was 10 and 24 months, respectively (p=0.0209) (Fig. 4).
DISCUSSION
Pancreatic cancer is a deadly disease with no effective therapy besides surgical resection. Although there have been many studies, none have yet elucidated the cause of poor prognosis in pancreatic cancer. Due to developments in molecular biology, there has been rapid progress in the understanding of the genetic aspects of cancers. Identifying genetic changes in cancer contributes not only to detecting the cause of cancer, but also to developing novel methods for diagnosis and treatment.
The mutation of p16 genes in pancreatic cancer is caused by homozygous deletion, point mutation, or methylation of the CpG island located in the p16 gene promoter region.6,9,10 The incidence of p16 gene mutation and protein expression in pancreatic cancer has been reported between 30 and 87%,8,10-12 with the wide range possibly caused by a difference in subjects or examinations. Prior studies have showed that compared to other tissues, pancreatic cancer cell lines had more p16 gene mutation; results were different based on mutation study methods and immunohistochemical staining. The results of this study, in which p16 protein expression was lost in 45.5% of patients, were similar to those of previous studies.
A recent study reported that p16 genes play an important role in the carcinogenesis of pancreatic cancer, and Hu et al.11 stated that comparison of p16 protein expression in normal pancreatic tissue, acute pancreatitis, cystic tumor of the pancreas, and pancreatic cancer produced a significant difference. Moskaluk et al.13 observed that the incidence of p16 mutation is high in early intraductal pancreatic cancer lesions with K-ras mutations, and stated that such mutations contributed to the development of infiltrating cancer. Another study, by Wilentz et al.14 had similar results, and reported that p16 genes played an important role in carcinogenesis of pancreatic cancer.
Many different results have been published regarding p16 gene association with clinicopathologic properties and survival rate. Bartsch et al.15 stated that median survival of cases with and without p16 mutation was 8.5 and 17 months, respectively. However, other studies,9,12 including our study, found no relationship between p16 gene overexpression and survival rate. Our results showed that loss of p16 expression is associated with lymphatic metastasis and pathologic stage. There are other reports showing that loss of p16 expression is associated with extent of histologic differentiation. However, no reports have yet demonstrated the association with lymphatic metastasis or tumor stage. Because lymphatic metastasis plays a critical role in discriminating stage II from stage III, we suggest that the stages are related to loss of p16 protein expression. Further studies using tissue from lymphatic metastasis are necessary.
Most of the p53 gene mutation in pancreatic cancer is caused by point mutation or loss of heterozygosity.3 The half-life of normal p53 protein is short (10-20 minutes), but that of mutant p53 protein is prolonged by several hours, making it possible to detect protein by immunohistochemical staining using monoclonal antibody.
The p53 mutation or p53 protein overexpression in pancreatic cancer is reported to be 37-76%.9,12,16-26 In our study it was 31.8%, lower than in previous studies. Some studies have reported association between p53 genes and the cell cycle, and have discussed the role of p53 in the carcinogenesis of pancreatic cancer.24 Zhang et al.25 stated that p53 mutation occurs in relatively early stages of carcinogenesis because p53 protein overexpression is observed in intraductal papillary adenocarcinoma. Ruggeri et al.19 reported similar results. However, researchers have proposed various results in the association between p53 mutation and clinicopathologic properties and survival rate. Many researches report that there is no association between p53 mutation and clinicopathologic properties,9,12,18-21,25 while Yokoyama et al.26 reported an association between p53 mutation and clinical stages. In this study, p53 protein overexpression was increased according to the extent of histologic differentiation.
Because some researches report that p53 protein expression is increased according to extent of histologic differentiation and p53 genes control cell cycle, it is probable that p53 mutation is associated with cell differentiation. In effect, further studies will be needed. Although there are many reports showing no relationship between mutation and survival, Yokoyama et al.,26 Nakamori et al.,22 and this study found that subjects with p53 protein overexpression had decreased survival; the varying results are probably due to diverse inclusion criteria and selection bias of the studies. Prospective randomized studies with more subjects are needed to clarify this issue.
Many studies observed pancreatic cancer cases in which p16 and p53 genes showed both variations.27 Naumann et al.28 reported that 77% of patients had variations either in p16 or p53 genes. In this study, although results were not shown, 6 cases (13.6%) had both loss of p16 protein expression and p53 overexpression, and 28 cases (63.6%) had either. However, concurrence of p16 protein loss and p53 overexpression failed to show clinical significance. A genetic model, including several genes associated with carcinogenesis could be applied to pancreatic cancer because many genes besides p16 and p53, such as K-ras and DPC4, have been implicated. The interactions between such genes has been identified to be related to carcinogenesis. In effect, further studies, including investigation of other tumor suppressor genes or oncogenes apart from p16 and p53, will contribute to the treatment of pancreatic cancer.





 XML Download
XML Download