

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Corticosteroids are widely used for the treatment of a variety of diseases such as asthma, inflammatory and allergic disorders, and other diseases affecting the gastrointestinal tract and central nervous system. Although corticosteroid treatment is often effective for these conditions, osteoporosis is one of its most serious complications. Because of the rapid loss of bone mineral density (BMD) and increase in fracture risk following the start of corticosteroid treatment, the early use of preventative measures against corticosteroid-induced osteoporosis should be considered.
Drugs used to treat corticosteroid-induced BMD loss include calcium, vitamin D, vitamin K, estrogen, calcitonin, fluoride, bisphosphonates, and parathyroid hormone (PTH). These therapies seem to maintain or increase BMD, and/or may possibly reduce the incidence of vertebral fractures.
The treatment of osteoporosis is performed based according to the practice of evidence-based-medicine (EBM). EBM incorporates information derived from the highest-quality investigations with clinical judgment and patient values to achieve optimal clinical management. A hierarchy of evidence exists, with meta-analysis representing the highest level, followed by randomized controlled trials (RCTs), which have long been considered the "gold standard" in regards to clinical investigations. This paper discusses the effect of several drugs on BMD of the lumbar spine and hip, which are clinically important sites, and the incidence of vertebral fractures in patients treated with corticosteroids, considering EBM in terms of the results of meta-analyses.
PREVENTION AND TREATMENT OF CORTICOSTEROID-INDUCED OSTEOPOROSIS
Pathogenesis of corticosteroid-induced osteoporosis
Corticosteroid-induced osteoporosis may result from the direct and indirect actions of corticosteroids on bone and calcium homeostasis. Direct effects include the suppression of intestinal calcium absorption, decreased renal tubular calcium reabsorption with increased urinary calcium excretion, and suppressed osteoblast function and decreased bone formation. Renal and intestinal losses of calcium result in the development of secondary hyperparathyroidism, which, in concert with the stimulation of parathyroid secretion and an increased sensitivity of bone cells to PTH, produces an increase in bone resorption and bone turnover.1 Several in vitro and ex vivo studies have indicated that excess corticosteroids promote apoptosis of osteoblasts and osteocytes, suppress the production of new osteoblasts and osteoclasts, and extend the life span of preexisting osteoclasts,2 which play main roles in the pathogenesis of corticosteroid-induced osteoporosis. Because of strong correlations between cumulative dose and loss of BMD, and between daily dose and risk of fracture, oral corticosteroid therapy using more than 5 mg (of prednisolone or equivalent) daily is reported to lead to a reduction in BMD and a rapid increase in the risk of fracture during the treatment period.3,4
Fractures in corticosteroid users have been suggested to occur because of BMD loss. However, corticosteroid users with fractures in fact have higher BMD than do in patients with age-related osteoporosis,5-7 suggesting a non-BMD-related mechanism responsible for inducing fractures. Kanis et al.8 reported that prior and current exposure to corticosteroids conferred an increased risk of fracture that was of substantial importance beyond that explained by measurements of BMD. Corticosteroid-induced osteoporosis is surmised to result partially from microarchitectural deterioration predisposing to bone fragility and fractures, similar to postmenopausal osteoporosis.
Recently, it was reported that the fracture risk increased rapidly (as early as three months) after the initiation of corticosteroid therapy, and that it reversed sharply toward the baseline after its discontinuation.9 The most logical explanation for the rapid onset and offset of fracture risk in corticosteroid-induced osteoporosis is suggested to be osteocyte apoptosis accompanied by a relative increase in resorption caused by prolongation of the life span of preexisting osteoclasts.2 Osteocyte apoptosis may lead to a deterioration of bone quality, with a rapid increase in the risk of fracture, because osteocytes play an important role in the maintenance of bone quality.2 As far as bone formation and resorption are concerned, because the key histological feature of corticosteroid-induced osteoporosis is suppressed bone formation, manifested as a reduction in trabecular bone thickness,10 the mechanisms of bone fragility and fractures in corticosteroid-induced osteoporosis may differ from those in postmenopausal osteoporosis, in which bone formation and resorption are increased and trabecular bone connectivity is reduced.
Prevention and treatment of corticosteroid-induced osteoporosis
Physicians should primarily avoid the unnecessary use of corticosteroids, and should make every effort to prevent fractures in patients who are initiating and continuing corticosteroid treatment.
The preservation of the osteocyte network seems to be an important mechanism by which bisphosphonates, calcitonin, and estrogen replacement therapy decrease bone fragility and fractures.11-13 However, because the prevention of osteoblast apoptosis predictably leads to more numerous and closely spaced osteocytes,14 the prevention of not only osteocyte apoptosis but also osteoblast apoptosis by treatment is a rationale approach for decreasing bone fragility and fractures. Although anti-resorptive agents such as bisphosphonates and anabolic agents such as PTH have the opposite effect on bone turnover, both agents have been shown to have potent anti-apoptotic effects on osteoblasts and osteocytes.13,14 Therefore, both anti-resorptive and anabolic agents may be the potential candidates for the treatment of corticosteroid-induced osteoporosis.
Several meta-analysis studies have reported the efficacy of vitamin D, calcitonin, fluoride, and bisphosphonates in patients treated with corticosteroids. Amin et al.15 suggested a hierarchy in efficacy among the agents used for the management of corticosteroid-induced osteoporosis with respect to their effect on lumbar spine BMD. Their meta-analysis results indicated that bisphosphonates were the most effective of the agents studied, in comparison with no therapy or treatment with calcium, and were more efficacious than either vitamin D (both activated vitamin D and other vitamin D formulations) or calcitonin (Table 1). These results were similar even when newer generations of nitrogen-containing bisphosphonates were excluded from analysis, and even when the trial characteristics were divided into two categories, i.e., prevention and treatment (treatment initiated within six months of corticosteroid therapy; Table 2). The efficacy of fluoride might be intermediate between that of bisphosphonates and that of vitamin D or calcitonin.15 The combined use of bisphosphonate and vitamin D has been emphasized, because the efficacy of bisphosphonates was enhanced when used in combination with vitamin D. When the outcome measure of interest was limited to the change in lumbar spine BMD, bisphosphonates were the most effective of the agents evaluated for managing corticosteroid-induced osteoporosis.
Several meta-analysis/systematic-review studies have reported the effects of vitamin D, calcitonin, and bisphosphonates on BMD of the hip as well as the lumbar spine and the incidence of vertebral fractures. Homik et al.16 reported that calcium and vitamin D preserved BMD at the lumbar spine with an increase of 2.6% compared with controls (calcium alone or placebo), but not at the hip, and did not reduce the incidence of fractures. Richy et al.17 also reported that activated vitamin D (alfacalcidol and calcitriol) maintained lumbar spine BMD, but did not reduce the incidence of vertebral fractures. Cranney et al.18 reported that calcitonin preserved BMD at the lumbar spine with an increase of about 3% compared to the placebo, but did not preserve BMD at the hip, and did not reduce the incidence of vertebral fractures in the first year of corticosteroid therapy. The researchers also suggested that the protective effect of calcitonin on BMD might be greater in patients who have been taking corticosteroids for more than three months. Homik et al.19 analyzed RCTs of bisphosphonates performed in patients who had been taking a mean corticosteroid dose of 7.5 mg/day or more, and reported that bisphosphonates preserved BMD at the lumbar spine and hip with an increase of 4.3% and 2.1%, respectively, compared to the placebo, but did not reduce the incidence of vertebral fractures. The results of these reports suggest that vitamin D, calcitonin, and fluoride stabilize lumbar spine BMD, while bisphosphonates stabilize both lumbar spine and hip BMD, with a less certain effect on hip BMD. The efficacy of vitamin D, calcitonin, fluoride, and bisphosphonates to reduce the incidence of vertebral fractures in patients exposed to corticosteroid remains to be established.
Efficacy of bisphosphonates for corticosteroid-induced osteoporosis
According to the results of the meta-analyses, bisphosphonates were considered to be the most effective of the agents evaluated for the treatment of corticosteroid-induced osteoporosis. That is, treatment with bisphosphonates resulted in a significant benefit for lumbar spine and femoral neck BMD in both prevention and treatment studies. A comparison of the efficacy of etidronate, alendronate, and risedronate based on the results of RCTs is of great interest.
Adachi et al.20 performed a pooled data analysis of the use of intermittent cyclical etidronate for the prevention and treatment of corticosteroid-induced BMD loss. They reported that intermittent cyclical etidronate (400 mg/day for two weeks every three months) was effective in preventing loss of lumbar spine and hip BMD (3.7% and 1.7% increases compared to placebo) and reducing the incidence of vertebral fractures in prevention studies and in slightly increasing lumbar spine BMD (4.8-5.4% increase compared to placebo) in treatment studies. Recently, Sato et al.21 examined the effect of intermittent cyclical etidronate combined with calcium + alfacalcidol on lumbar spine BMD and the incidence of vertebral fractures in Japanese men and pre- and postmenopausal women who were taking >7.5 mg of prednisolone daily for at least 90 days. Intermittent cyclical etidronate therapy (200 mg/day for two weeks every three months) combined with calcium + alfacalcidol for three years increased lumbar spine BMD by 4.8%, while calcium + alfacalcidol alone increased it by only 0.4%. Among men and pre- and postmenopausal women, postmenopausal women showed the greatest increase in lumbar spine BMD (10.1%). However, there was no significant reduction in the incidence of vertebral fractures by intermittent cyclical etidronate combined with calcium + alfacalcidol compared to calcium + alfacalcidol alone. Nakayamada et al.22 also studied the efficacy of intermittent cyclical etidronate (200 mg/day for two weeks every three months) combined with alfacalcidol for lumbar spine and hip BMD in Japanese men and premenopausal women starting high-dose corticosteroid treatment (minimum starting dose 30 mg/day prednisolone or equivalent dose of a methylprednisolone derivative). The percent changes in lumbar spine and hip BMD were -10.3% and -2.5%, respectively, in the alfacalcidol group, and -4.5% and 2.3%, respectively, in the intermittent cyclical etidronate combined with alfacalcidol group. There was no significant difference in bone turnover markers between the two groups. Intermittent cyclical etidronate could retard and prevent high-dose corticosteroid-induced BMD loss at the lumbar spine and hip.
Adachi et al.23 reported on the efficacy of alendronate for lumbar spine and hip BMD and the incidence of vertebral fractures in men and pre- and postmenopausal women continuing to receive at least 7.5 mg of prednisone or equivalent daily. Alendronate therapy (5, 10, or 2.5/10 mg daily) for two years reduced the levels of turnover markers (urinary N-terminal telopeptides of type I collagen and serum alkaline phosphatase), increased lumbar spine BMD by 2.8 to 3.9% with a significant difference from the placebo (0.8% decrease), and reduced the incidence of vertebral fractures (0.7% in the alendronate group versus 6.8% in the placebo group).
Eastell et al.24 examined the effect of risedronate on lumbar spine and hip BMD in postmenopausal women with rheumatoid arthritis requiring long-term corticosteroid therapy at >2.5 mg/day prednisolone. Risedronate therapy (2.5 mg daily) for 97 weeks preserved lumbar spine BMD with an increase of 1.4% (1.6% decrease in the placebo group), but did not prevent hip BMD loss compared to the placebo (1.0% and 3.6% decreases in the risedronate and placebo groups, respectively). Cohen et al.25 studied the efficacy of risedronate for lumbar spine and hip BMD and the incidence of vertebral fractures in men and pre- and postmenopausal women who were initiating long-term corticosteroid treatment. Risedronate therapy (2.5 or 5 mg daily) for 12 months preserved lumbar and hip BMD compared to placebo controls (-0.1 to 0.6% versus -2.8% at the lumbar spine and -0.4 to 0.8% versus -3.1% at the hip), but did not reduce the incidence of vertebral fractures. Reid et al.26 also studied the efficacy of risedronate in men and pre- and postmenopausal women receiving high-dose oral corticosteroid treatment (prednisone ≧ 7.5 mg/day or equivalent) for six or more months. Risedronate therapy (2.5 or 5 mg daily) for 12 months increased lumbar BMD with an increase of 1.9 to 2.9% (0.4% in the placebo group), preserved hip BMD by -0.2 to 1.8% (-0.3% in the placebo group), and reduced the incidence of vertebral fractures by 70% in the two active treatment groups combined.
For pre- and postmenopausal women as well as men, where they were included in the studies, etidronate, alendronate, and risedronate are considered to have similar benefits for lumbar spine and hip BMD in patients who are initiating or receiving corticosteroid treatment. However, the anti-fracture efficacy in the spine seems to be less certain, although some RCTs did report efficacy. According to the results of RCTs, etidronate, alendronate, and risedronate could be candidates for preventing vertebral fractures in patients treated with corticosteroids.
Efficacy of other agents for corticosteroid-induced osteoporosis
Estrogen
Hall et al.27 studied the efficacy of hormone (estrogen) replacement therapy (HRT) for lumbar spine and hip BMD in postmenopausal women with rheumatoid arthritis treated with low-dose corticosteroids. Twenty-four months of HRT increased lumbar spine and hip BMD by 3.8% and 1.6%, respectively, while calcium supplementation alone decreased them by 1.2% and 0.6%, suggesting that HRT was effective for preserving lumbar spine and hip BMD in postmenopausal women taking low-dose corticosteroids.
Parathyroid hormone
PTH is known to be a potent anabolic agent. Lane et al.28 reported changes in BMD after 12 months of daily injections of human PTH (1-34) [hPTH (1-34)] in postmenopausal women with osteoporosis treated with corticosteroids and HRT. Twelve months of PTH estrogen therapy increased lumbar spine BMD by 11.9% and preserved hip BMD (3.3% increase), while estrogen alone preserved both lumbar spine and hip BMD (1.1% increase and 1.6% decrease, respectively). These results suggest that PTH markedly increased lumbar spine BMD and preserved hip BMD in postmenopausal women with corticosteroid-induced osteoporosis who were taking HRT. The large increase in lumbar spine BMD due to PTH therapy offers hope that corticosteroid-induced BMD loss may be reversed.
Vitamin K2
Vitamin K2 is available in Japan. Vitamin K2 is a cofactor of γ-carboxylase, which converts glutamic acid residues in osteocalcin to γ-carboxyglutamic acid, and is, therefore, essential for the γ-carboxylation of osetocalcin.29,30 Because corticosteroid therapy decreases serum osteocalcin levels,31 vitamin K2 may be effective for the treatment of corticosteroid-induced osteoporosis.
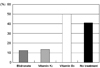
Several studies have reported the efficacy of vitamin K2 (menatetrenone) for the treatment of corticosteroid-induced osteoporosis in Japan. Tanaka and Oshima32 investigated the risk factors for vertebral fractures caused by corticosteroid-induced osteoporosis in 103 patients with collagen diseases, including rheumatoid arthritis, who were under treatment with vitamin K2, etidronate (200 mg/day for two weeks every three months), or active vitamin D3, or who were not under any medication to improve bone metabolism for two years. They demonstrated that the independent risk factors for the appearance of new vertebral fractures were age (Odd' ratio 2.03, p=0.008 per 10 years increase), increase in glucocorticoid dosage (Odd's ratio 6.62, p=0.018), prevalence of vertebral fractures (Odd's ratio 7.90, p=0.028), low lumbar spine BMD (Odd's ratio 1.47, p=0.0003 per 5% decrease compared to the young adult mean), treatment with therapeutic agents, vitamin K2 and etidronate (Odd's ratio 0.03, p=0.003 and Odd's ratio 0.02, p=0.002, respectively), and gender (male) (Odd's ratio 10.9, p=0.011). In particular, treatment with vitamin K2 and etidronate significantly reduced the risk of vertebral fractures (Odd's ratio 0.03, p=0.003 and Odd's ratio 0.02, p=0.002, respectively; Fig. 1).
Tanaka and Oshima33,34 also showed the therapeutic effects of etidronate (200 mg/day for two weeks every three months), vitamin K2 (menatetrenone), and active vitamin D3 in patients with corticosteroid-induced osteoporosis, focusing on the incidence of new vertebral fractures, in 136 patients with collagen diseases other than rheumatoid arthritis. During the two-year study period, new vertebral fractures were observed in 31% of patients in the non-treatment group. The incidence of vertebral fractures was significantly reduced in the vitamin K2 and etidronate treatment groups (13% and 11%, respectively), but was increased in the vitamin D3 treatment group (41%), suggesting that vitamin K2 as well as etidronate may be efficacious for preventing vertebral fractures in patients with corticosteroid-induced osteoporosis.
Although only small numbers of published data are available for vitamin K2 as a treatment for corticosteroid-induced osteoporosis, we expect that the efficacy of vitamin K2 will be demonstrated in patients treated with corticosteroid who have a high serum level of undercarboxylated osteocalcin and/or low serum level of osteocalcin, taking into consideration the action of vitamin K2 on osteocalcin.
Based on the report that showed the additive beneficial effects of vitamin K2 to those of a bisphosphonate for postmenopausal osteoporosis,30,35 the efficacy of combined treatment with bisphosphonates and vitamin K2 for the incidence of osteoporotic fractures may be considered for glucocorticoid-induced osteoporosis.
CONCLUSIONS
A study of meta-analysis representing the highest level in a hierarchy of evidence showed that bisphosphonates were the most effective agent in increasing lumbar spine BMD in patients exposed to corticosteroid, and their efficacy was enhanced when used in combination with vitamin D.15 RCTs representing the second level in a hierarchy of evidence showed that bisphosphonates stabilized BMD not only in the lumbar spine, but also in the hip, and that PTH markedly increased lumbar spine BMD. Some RCTs also demonstrated the anti-fracture effects of etidronate, alendronate, and risedronate in the spine. Further RCTs of fracture prevention conducted on a large number of patients and their meta-analysis are needed to confirm the efficacy of bisphosphonates, PTH, or possibly other agents in preventing vertebral and nonvertebral fractures.


 XML Download
XML Download