

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
In lung cancer, bone metastasis is present in more than 20% of patients at initial presentation1 and accurate evaluation of metastatic bone involvement is important in determining the therapeutic strategies. Therefore, reliable methods to detect metastasis are required for tumor-staging and follow-up of the disease. Bone metastasis is usually determined initially with bone scintigraphy screening, and further evaluation with bone X-ray and/or magnetic resonance imaging (MRI). Bone scintigraphy is sensitive for the detection of bone metastasis.2,3 However, the false positive rate is reported to be 40-50%.3 Plain radiography is specific but insensitive because nearly 50% of bone mineral must be lost for bone metastasis to be detected.4 MRI, one of the best diagnostic techniques, is inadequate for initial screenings because of its high cost. Thus, the development of precise and useful markers is needed. In recent years, new biochemical markers of the remodeling process in bone have become available. Among the new biochemical marker of bone turnover, bone specific alkaline phosphatese reflects bone formation, while urinary deoxypyridinolie (DPD), and urinary pyridinoline cross-linked N-telopeptides of Type I collagen (NTx) reflect bone resorption. These biochemical markers of bone turnover are believed to be useful in the diagnosis of many metabolic diseases5,6 and have been reported to be valuable in investigating bone metastasis from breast cancer,7 prostate cancer8,9, and multiple myeloma.10 In this study, we investigated the usefulness of urinary pyridinoline cross-linked N-telopeptides of Type I collagen (NTx), urinary deoxypyridinoline (DPD), serum alkaline phosphatase (ALP) in the assessments of bone metastasis in patients with lung cancer.
MATERIALS AND METHODS
Patient population
One hundred fifty one ambulatory patients with lung cancer who were admitted to the Yonsei University College of Medicine, Severance Hospital in Seoul, Korea between October 2002 and July 2003 were studied. Thirty-three patients with bone metastasis and 118 patients without bone metastasis were included in this study. None of the patients in the study had received any antineoplastic therapy (Chemotherapy or radiotherapy).
The median age was 62 years (range, 28 to 84 years); 105 patients were male and 46 patients were female. The diagnosis of lung cancer was confirmed cytologically or histologically. The patients who had humoral hypercalcemia associated with malignancy, hyperparathyroidism, hypoparathyroidism, hyperthyroidism, traumatic fracture (within 6 months), renal failure, or previous bisphosphonate treatment were excluded from this study. All patients gave their informed consent to the diagnostic procedures.
Bone metastasis evaluation: All patients were evaluated for bone metastasis by bone scintigraphy. A total of 25 mCi 99mTechnetium methylene diphosphonates (MDP) was injected intravenously, and front and back images of the whole body were taken after 3 hours. The apparatus used was a double-detector gamma camera (VERTEX, ADAC Co., CA, USA). Bone scintigraphy was read by two radiologists and classified into either a bone metastasis-positive or a negative group. When the bone scintigraphic interpretation differed among radiologists, positive scans were further assessed by additional radiographs; computerized tomography, magnetic resonance imaging, positron emission tomography or bone biopsy, except when the increased uptake was recognized as being due to a benign condition.
Biochemical analysis: Urine NTx, DPD and serum ALP were measured within 10 days after the bone scintigraphic examination in all cases. For NTx and DPD measurements, a 2-hour urine collection was obtained after first morning urine was voided, and then preserved frozen at -20℃. Urinary concentration of DPD was determined using a radioimmunoassay according to the manufacturer's instructions (Gamma-BCT DPD kit; Immunodiagnostic Systems, Boldon, England) and urinary NTx was calculated by competitive immunoassay (Vitros™ NTx reagent pack; Ortho-clinical Diagnostics, Inc., Rochester, NY). Alkaline phosphatase was assayed by Beckman LX® 4201 automated analyzer (Beckman Coulter Inc, CA, USA) using p-nitrophenyl phosphate as substrate. The values for urinary DPD and NTx were corrected for urinary creatinine to overcome confounding variables such as body mass index and urine dilution. The reference ranges for DPD and NTx taken from normal populations were 2.5-5.5 and 6-94 µmol/mol creatinine, respectively. The reference range for ALP was 38-115 IU/L.
The statistical analysis: The difference between the mean values of the two groups was evaluated by Student's t-test and linear regression with Pearson's correlation coefficients. The relative effectiveness of the diagnostic tests was assessed by plotting the true-positive (sensitivity) vs false-positive (1-specificity) ratios on receiver operating characteristic (ROC) curves. To evaluate the independent contributions of DPD, NTx, and ALP in predicting bone metastasis, correlation coefficients were calculated. A p value < 0.05 was considered statistically significant.
RESULTS
Sixteen cases (10.7%) of bone scintigraphic interpretation differed among radiologists. The discrepancies found were further assessed by additional radiographs; computerized tomography (5 cases), magnetic resonance imaging (8 cases), positron emission tomography (3 cases).
Descriptive statistics of bone markers from individual cancer patients with and without clinical evidence of bone metastasis are presented in Table 1. The mean urinary concentrations of DPD in lung cancer patients with and without bone metastasis were 13.1 ± 1.1 µmol/mol creatinine and 7.4 ± 0.4 µmol/mol creatinine, respectively (p value=0.001). The mean urinary concentrations of NTx in lung cancer patients with and without bone metastasis were 120.3 ± 23.6 µmol/mol creatinine and 50.7 ± 2.3 µmol/mol creatinine, respectively (p value=0.015). Serum marker of bone formation, ALP, also displayed a higher mean concentration in the group with bone metastasis than in the group without bone metastasis (p value=0.0006). As shown in Fig. 1, plotting the individual patient's values for DPD, NTx, and ALP showed that a majority of lung cancer patients with bone metastasis had high concentrations. In addition, 4% (4 of 118 patients) of the patients without bone metastasis had NTx concentrations greater than the upper limit of the reference value. Similar patterns were observed with DPD (64%) and ALP (15%).
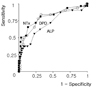
Fig. 2 shows the ROC curves of DPD, NTx, and ALP for the diagnosis of bone metastasis. NTx showed the best curve characteristics among the three bone markers, followed by DPD, ALP. For NTx, the sensitivity (73%) and specificity (84%) was seen at the cut-off level of 73 µmol/mol creatinine. For DPD, the sensitivity (82%) and specificity (72%) was seen at the cut-off level of 8.3 µmol/mol creatinine. For ALP, the sensitivity (70%) and specificity (70%) was seen at the cut-off level of 90U/L. The areas under the ROC curve were 0.82, 0.79, and 0.71, respectively.
DISCUSSION
The initial diagnosis of bone metastasis is usually made with bone scintigraphy, but its use is limited due to high cost, false positive rate, and the inconvenience of using radioactive substances. Repeatedly monitoring bone metastasis with it during treatment cause even more problems. Until now, serum alkaline phosphatase has been used as an alternative tool to monitor bone metastasis, but it lacks specificity. ALP is produced not only by osteoblasts but also by various organs, such as the liver, small intestine and placenta, and elevation of its level is not specific to identifying bone metastasis. Bone-specific alkaline phosphatase, which is an isoenzyme of ALP derived from bone, seems to be more specific in bone metastasis than ALP.11
Urinary hydroxyproline, another marker of bone metastasis, also lacks specificity because it exists not only in bone, but also in elastine and complement, and its measurement is interfered by diet. More convenient and less expensive method with good sensitivity and specificity to detect bone metastasis has been sought.
Several new biochemical markers of bone turnover have been developed, and they are being tested as a marker of bone metastasis. Deoxypyridinoline (DPD), one of such markers, is distributed mostly in bone collagen, has a higher specificity for bone than pyridinoline, is excreted in urine, and is not affected by diet, not metabolized internally. Therefore, it is expected that its measurement in urine may be more useful for monitoring bone resorption than pyridinoline. The pyridinium cross-links in DPD are nonreducible collagen cross-links within the extracellular bone. They are released with the breakdown of bone and appear to show promise as specific markers of bone degradation. Pyridinoline is abundant in bone and cartilage, whereas DPD appears to be present in significant amounts only in bone.12 The cross-linked N-telopeptides are Type I collagen breakdown products that are specific for bone discovered in the urine.
They elevate in patients with various metabolic bone diseases, including Paget's disease, osteoporosis, and primary hyperparathyroidism,13 and it was reported that they were useful for monitoring patients with metastatic bone disease originating from prostate carcinoma,8,9 and breast carcinoma.7 Demers et al., evaluated seven biochemical markers of bone formation and resorption in 94 patients with malignant disease including bone metastasis, and among those markers urine NTx showed the most promising result,13 which is compatible with our results.
However, in patients with lung carcinoma, there were little reports showing the clinical utility of these new markers.14-16 We found that lung cancer patients with bone metastasis had significantly higher concentrations of urine DPD, NTx, and serum ALP than patients without metastasis. Among those markers, urinary NTx was the most reliable biochemical indicator of bone metastasis.
We also noted that some of patients without documented bone metastasis exceeded the upper reference limit for this assay. If this reflected subclinical bony involvement not yet resolved by bone scintigraphy, these markers might detect disseminated disease earlier than by bone scintigraphy. This would alter the treatment strategy and improve the disease morbidity caused by bone metastasis, but further studies are needed to confirm this. In addition, an important advantage of these biochemical bone markers over that of bone scintigraphy lie in their ability to monitor bone metastasis more quickly.
During the study we found that these new markers were better than alkaline phosphates, but also had some problems. Significant differences in urine NTx and DPD were observed between the bone metastasis-positive and negative groups, but the variance in values between the 2 groups overlapped, as shown in Fig. 1. These results illustrated the difficulties associated with diagnosing the presence or absence of bone metastasis solely by urinary analysis of NTx and DPD.
We conclude that NTx was superior to other biomarkers such as ALP, DPD in detecting bone metastasis in patients with lung carcinoma. The application of these results can be applied to indicate the need to perform other radiographic evaluations such as bone scintigraphy. We feel that further studies with larger numbers and additional information on follow up are needed.



 XML Download
XML Download