

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Snellen visual acuity and other similar recognition acuity tests are performed under high contrast photopic conditions (80-320cd/m2). However, the functional vision is influenced by ever-changing environment and is apt to be exposed to low contrast condition in everyday life. While the letter acuity test generally indicates the patient's ability to see small details in the environment, contrast sensitivity test (CST) measures the ability to see large details as well. In many ways, contrast sensitivity test is expected to be more useful for the accurate evaluation of the visual function with three to five times sensitivity in daily life.1,2 Decreased contrast sensitivity at high spatial frequencies occurs in the disorders associated with decreased Snellen visual acuity.3 So the CST should be useful in charting the progress of a pathological condition or its response to a therapeutic regimen.4,5
The Visual Capacity Analyzer (ACV, designed by Philippe Liebaert, 1996) which can fully assess visual capacity in the medical field uses computerized tools to investigate the visual performance. The sensitivity of the morphoscopic contrast test using the ACV explores the full range of shapes of visual performance as well in photopic and mesopic conditions. The contrast ranges consist from 1 to 99% and the frequencies range from 0.6 to 30cpd by Landolt ring. The ease and simplicity of the ACV test makes it ideal for measuring contrast sensitivity functions in children less than 10 years of age.6
The contrast sensitivity function under mesopic luminance has rarely been measured and reported in normal or amblyopic eyes. A comparison between the normal eyes and the corresponding amblyopic eyes showed that the contrast sensitivity functions decreased in the amblyopic eyes under mesopic conditions.6 We performed this study to verify the changes of mesopic and photopic contrast sensitivity function of sound eye whose visual acuity was kept the same after occlusion therapy in the amblyopic children.
MATERIALS AND METHODS
Fourteen sound eyes of amblyopic children (mean; 7.67 years; S.D., 1.50 years) who kept their sound visual acuity the same after the occlusion therapy were tested. The children had 6 hours of part-time patch therapy for 3 months prior to this examination. Among 14 amblyopic children, 8 were anisometropic and 6 were strabismic amblyopes.
Using ACV, which measures the minimal contrast level from low to high spatial frequencies, the contrast sensitivity of sound eye was measured, under both photopic (maximum luminance) and mesopic (3cd/m2) condition, before occlusion therapy and after 3 months of occlusion therapy.
A standard fifteen inch monitor was used and the horizontal distance of one meter between the monitor and the eye was adjusted. Tests have been performed in a dark room with the computer monitor as only light source. In these conditions, the investigator easily operated the ACV. The optotypes selected for the tests were Landolt rings.
The minimum contrast levels that allow the examinee to read accurately all the different sized letters displayed on the screen were measured at eleven different spatial frequencies ranging between a low spatial frequency (0.6 cyc/deg) and a high spatial frequency (30.0 cyc/deg). The contrast levels changed between 0.1% and 100%. Both eyes were tested twice under both mesopic and photopic conditions. The measured levels were calculated in terms of dB unit to be used for statistical analyses. Unless stated otherwise, the results of the two tests on each eye were averaged to give a single contrast sensitivity function.
The data were analyzed with paired t-test of the SAS (statistical analysis system) program.
RESULTS
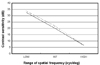
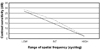
The average of best corrected visual acuity in their amblyopic eyes improved to 20/30 from 20/40, while the average of best corrected visual acuity in their sound eyes was same as 20/25 after 3 months of occlusion compared with before of occlusion. Comparing the contrast sensitivity function of sound eye after the occlusion therapy to that of before occlusion, there was no statistical difference in photopic condition. (Table 1, Fig. 1) When it comes to mesopic condition, the contrast sensitivity function decreased particularly in the intermediate spatial frequency level after the occlusion therapy (3.0-13.0 cyc/deg, p=0.028) (Table 2, Fig. 2).
DISCUSSION
There have been many studies on the contrast sensitivity functions of amblyopes, but they were usually performed under photopic conditions. It is generally considered that the photopic contrast sensitivity is related to the visual functions of the amblyopic eye.7,8 But Howell et al. found a poor relationship between photopic contrast sensitivity function and visual acuity in the amblyopic eye on the contrary.9
This is the first report to measure the mesopic contrast sensitivity function of sound eyes of occlusion therapy in childhood amblyopia. The mesopic contrast sensitivity curve showed similar pattern to the photopic contrast sensitivity curve before occlusion in this study. But the sound eyes showed the decrease of the contrast sensitivity functions in the intermediate spatial frequencies under mesopic conditions after occlusion therapy. It is conceivable that the mesopic contrast sensitivity is sensitive in detection of the functional change of sound eye after occlusion therapy.
The pediatric ophthalmologists usually examine the visual acuity of a sound eye to monitor the occlusion amblyopia, while the occlusion therapy is performed. The first developing amblyopia was reported to be related with the decrease of fixation ability in the sound eye in a binocular fixation test prior to the reduction of visual acuity during the penalization therapy for strabismic amblyopia.10 These facts suggested that occlusion amblyopia was not the result of deviation but the reversal of the eye used for fixation. Therefore further studies on the relations of the various tests including mesopic contrast sensitivity function to compare the sensitivity to detect the change of sound eye are requested.
The amblyopic eye may influence on the contrast sensitivity of the dominant eye through interocular interactions after occlusion. Interocular transfer was found to be dependent upon the sensitivity ratio of the non-amblyopic to the amblyopic eye.11 This process may help to minimize interocular contrast sensitivity differences and maximize binocular vision to improve the therapeutic effect of occlusion therapy.
The mesopic contrast sensitivity was reported to be low in the amblyopic eyes compared with in the sound eyes measured with ACV.6 The result supports that it may be more affected at intermediate frequency than at another frequency levels after occlusion.
The two types of amblyopia at intermediate frequencies are different in visual physiology, but we did not compare the mesopic contrast sensitivity function according to the subtype of amblyopes due to small sample size. It was in the amblyopic condition (decreased visual acuity) that we intended to focus to evaluate the mesopic contrast sensitivity functions of the sound eyes in this study. The other previous studies on the contrast sensitivity functions included the amblyopic patients regardless of the cause of amblyopia. The investigation on the mesopic contrast sensitivity functions according to the causes of amblyopia may be helpful in understanding of the physiology of contrast sensitivity functions of both eyes.


 XML Download
XML Download