

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
The majority of Charcot-Marie-Tooth 1(CMT1) patients possess DNA rearrangements, which are the molecular causes of their disease. A 1.5-Mb tandem duplication, the CMT1A duplication, accounts for approximately 70 percent of CMT1 cases, and a deletion of the same 1.5-Mb region in chromosome 17p11.2 is found in >85 percent of patients with HNPP. The CMT1A duplication and HNPP deletion result from unequal crossing-over and reciprocal homologous recombination involving a 24-Kb repeat-CMT1A-REP-which flanks the 1.5-Mb region. A meiotic recombination hotspot occurs within CMT1A-REP. The majority of the de novo duplication and deletion events occur during male germ cell meiosis. The CMT1A and HNPP phenotypes result from a gene dosage effect. CMT1A is due to trisomic overexpression of the peripheral myelin protein-22 gene (PMP22) whereas HNPP results from the monosomic underexpression of PMP22. Moreover, in rare cases PMP22 point mutations can cause disease in patients without the CMT1A duplication or the HNPP deletion.1
In molecular genetic testing for the CMT1A duplication and the HNPP deletion, several approaches are available. Molecular diagnosis by hybridization-based methods include; Southern blotting,2-5 quantitative photostimulated luminescence (PSL) imaging,6-9 and pulse-field gel electrophoresis (PFGE).2,5,10-12 Less frequently used methods include fluorescence-in situ hybridization (FISH),13,14 polymorphic markers,12,15 repeat (REP-) PCR,16-18 and endpoint quantitative PCR.19,20 But, these methods have several disadvantages for the diagnosis of CMT1A and HNPP.
In this study, we describe a rapid real-time quantitative PCR devised to assess gene copy number for the identification of DNA duplication or deletion occurring in CMT1A or HNPP, and we compare the results obtained with REP-PCR.
MATERIALS AND METHODS
Subjects and DNA extraction
Six patients with CMT1A and 14 patients with HNPP (confirmed by REP-PCR), 16 suspicious CMT1A and 13 suspicious HNPP patients with negative REP-PCR, and 15 normal controls were studied. Genomic DNA was extracted from EDTA-treated blood using the MagNa Pure LC DNA isolation kit and instrument (Roche), according to the manufacturer's instructions. DNA analysis was carried out with 'informed consent'.
Real-time quantitative PCR
Primers and probes used for real-time quantitative PCR were designed using LightCycler Probe Design Software version 1.0 (Roche). The amplified fragment (202 bp), including exon 5 of the PMP22 gene, was obtained using forward primer 5'-ACC CAG TGC ATC CAA C-3' and reverse primer 5'-ATC CAT AGC ACC ATT TCA AAG-3'. The sequence of the sensor probe was 5'-CGG CTT GTG GCA TTG GCA-Fluorescein-3', and the sequence of the anchor probe 5'-LCRed 640-CTT GCC CTT ACA GGT GGA GTA TCT-3'. The primers and probes of the β-globin gene in LightCycler Control DNA kit (Roche) were used as reference. Amplification was carried out using the LightCycler FastStart DNA Master Hybridization Probe kit (Roche) in a standard PCR containing; 0.5µmol/L of each primer and 0.2µmol/L of each probe in a 20µL final volume containing 2µL of sample. The cycling program consisted of an initial denaturation at 95℃ for 10 min, and 45 cycles of 95℃ for 10 sec, 58℃ for 10 sec, and 72℃ for 9 sec. Amplifications of PMP22 and β-globin were performed simultaneously in each capillary tube. Each test was repeated three times.
Calculating the gene copy number
Using a comparative threshold cycle (Ct) method, as previously described by Livak,21 and β-globin as a reference gene, the gene copy number by PMP22 gene duplication or deletion was quantified and calculated.
RESULTS
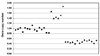
The amplification curves for PMP22 and the β-globin gene are shown in Fig. 2. The Ct values of PMP22 and of the β-globin gene were almost the same in the normal sample, whereas the Ct values of PMP22 in CMT1A and HNPP were decreased or increased, respectively, versus that of β-globin in the amplification curve. The PMP22 duplication ratio in two CMT1A patients, confirmed by REP-PCR, ranged from 1.35 to 1.74, the PMP22 deletion ratio in 14 patients with HNPP, as confirmed by REP-PCR, ranged from 0.41 to 0.53 and the PMP22 ratio in the controls ranged from 0.81 to 1.12 (Table 1). The standard deviations of Ct were 0.22, 0.18 and 0.24 in CMT1A, HNPP and controls, respectively. Six patients with CMT1A and the 14 patients with HNPP, as confirmed by REP-PCR, were positive by real-time quantitative PCR. Among the 16 suspicious CMT1A and 13 suspicious HNPP patients, with a negative REP-PCR, 2 and 4 samples, respectively, were positive by realtime quantitative PCR. Therefore, the real-time quantitative PCR method can be more detected 50% (2/4) of the CMT1A patients and 22.2% (4/18) of the HNPP patients with cross-over in CMT1A-REP. The measured copy numbers of the 15 normal controls, and in the 2 CMT1A and 14 HNPP patients are shown in Fig. 3. No overlap of copy number was found between CMT1A or HNPP patients and the controls.
DISCUSSION
At least nine loci for CMT1 and four for CMT2 have been identified by genetic linkage studies. Six of the genes associated with CMT1, and recently one gene for CMT2, has been identified. Although at least eight loci are associated with the aCMT1 phenotype, 70 to 90% of patients possess the causative CMT1A duplication. Deletion of the same genomic segment that is duplicated in CMT1A leads to a clinically distinct neuropathy-HNPP.1 Recombination events occur within the 1.7 Kb hotspot located between an EcoRI site, unique to the proximal CMT1A-REP, and a NsiI site, unique to distal CMT1A-REP. It has been reported that the recombination rate in hotspot region ranges from 75 to 87% in a population-dependent manner.1 In the present study, the recombination rate in the hotspot region was about 73% (16/22), which is similar to that obtained in other populations.
Several methods for detecting the CMT1A duplication and the HNPP deletion are available currently. Recently, the real-time quantitative PCR method has been used to detect haploidy and triploidy in genetic diseases and cancer.22-25 Detection of the PMP22 duplication and deletion by real-time quantitative PCR using TaqMan probes has been know as a fast method allowing to be diagnosed in 2 hr. However, specific probes are requiredin real-time quantitative PCR using TaqMan probes.
In the present study, this method also can be more found 27% (6/22) of duplication and deletion and is more sensitive than REP-PCR. However, many more samples should be tested for CMT1A duplication ratio. For mutation studies in the PMP22 gene, P0 gene (CMT1B), connexin32 gene (CMT1X),26 or another subtype of CMT is needed in samples without duplication or deletion.27 One case of CMT1A patient with 1.87 of gene copy number was presumed homozygote duplication, but it should be confirmed by other reference method e.g. FISH.
The reaction efficiencies varied in the different experiments, thus it may not be possible to obtain similar efficiencies for both control and target markers. This limitation also affects highly accurate systems such as the LightCycler instrument. But the gene dosage test in the method described is feasible and more accurate. In this study, the mean CV of the Ct value of the PMP22 and β-globin genes was < 2.0% in between run. Therefore, it appears that results of real-time quantitative PCR were accurate and reproducible.
In conclusion, real-time quantitative PCR is both more sensitive and more accurate than REP-PCR in terms of the detection of PMP22 duplications or deletions. It is also faster and easier than other currently available methods and clearly differentiates gene dose. Therefore, real-time quantitative PCR method may be useful for diagnosing CMT1A and HNPP, and may be applied to the diagnosis of any disease caused by gene dosage changes.



 XML Download
XML Download