

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Myocardial single photon emission computed tomography (SPECT) has emerged as an important noninvasive diagnostic and prognostic method for the assessment of patients with suspected coronary artery disease (CAD) (1, 2). However, the effect of respiratory motion on myocardial perfusion imaging (MPI) may lead to misinterpretation of images, especially for regional and global left ventricular (LV) function (3, 4). Motion of the heart due to respiration can be up to 18 mm in the cranio-caudal direction and motion is less in the horizontal and vertical directions (5, 6). Motion may cause blurring artifacts, decreasing image resolution and consequently a limitation in the detection of regions with reduced tracer uptake in MPI studies. Additionally, motion may affect the quantitative parameters acquired by the use of gated myocardial perfusion SPECT (GSPECT) (7-9). In previous studies, the use of respiratory gating showed promising findings with the use of computed tomography (CT), magnetic resonance imaging (MRI) as well as radiotherapy (10-12). Several studies have presented different approaches for the detection of respiration related myocardial motion both on positron emission tomography (PET) as well as SPECT imaging modalities (13-18).
Recently, respiratory gating has been introduced as a novel technical approach for correcting MPI distortions that originate from respiration motion (3, 4, 8, 14, 19). Respiratory gating provides different frames that correspond to the different parts of the respiratory cycle (13). Acquisition requires a real-time system to estimate respiratory gating according to the respiratory cycle. The respiratory gating parameters are determined by monitoring respiratory motion of patients by means of the use of external respiration signal markers. Correction of perfusion images distorted by respiration motion has been performed mainly using list-mode acquisition (5, 8, 20). A commercially available respiratory gating system, which uses an external respiration signal as a real-time position management (RPM) system has been most frequently discussed in previous publications (21, 22). In this study, we performed simultaneous respiratory and cardiac gated SPECT (RC-GSPECT) with concurrent correction of undesirable respiratory motion with the use of high cranio-caudal amplitudes. Furthermore, we examined if this approach was clinically relevant when compared with the use of routine GSPECT studies and both visual and quantitative analysis of myocardial perfusion and function were assessed.
MATERIALS AND METHODS
Patients
Twenty-six patients (15 female, 11 male; mean age, 65 ± 10 years; age range, 46-79 years) with known or suspected CAD were enrolled to undertake both stress and rest RC-GSPECT and GSPECT MPI between May and October 2007 in the Department of Nuclear Medicine and Endocrinology, St. Vincent's Hospital, Linz, Austria.
Exclusion criteria were a history of myocardial infarction, progressive cardiomyopathy, active lung disease and dyspnea, cardiac arrhythmia and musculoskeletal disease causing pain and inability to lie still for both acquisitions. Additionally, patients with studies that showed significant extracardial hot spots and non-respiratory body motion were excluded from the study.
An institutional ethics committee approved the study and all patients gave written informed consent to participate in this study.
Data Acquisition
A two-day stress-rest imaging protocol was performed for all patients. Pharmacological stress testing was performed after injection of 0.56 mg/kg dipyridamole for four minutes followed by administration of 740 MBq 99mTc-Tetrofosmin three minutes after the termination of the dipyridamole injection. The rest phase was performed on the subsequent day with the same dose of radiotracer. Imaging was performed 45 minutes after radiotracer injection for both stress and rest GSPECT and subsequently for use of the RC-GSPECT method. All acquisitions were performed in the SPECT mode by use of a GE DST-Xli dual-head gamma camera (GE Healthcare, Buc, France), equipped with parallel-hole low energy-high resolution (LEHR) collimators. For each study, 32 projections of an accepted acquisition time of 50 seconds per projection were acquired with a 64 × 64 matrix size and 1.33 zoom factor (pixel size = 0.66 cm) in an elliptical orbit of 180 degrees (45-degrees, right anterior oblique to left posterior oblique-RAO-to-LPO) in the step and shoot mode. Cardiac gating was performed using the detection of R wave for the monitoring of different phases of the cardiac cycle (1, 2). Gating was performed as 8 frames per cycle. The acceptance window for the R-R interval was set to 20%. Image reconstruction and processing by use of the ordered-subset expectation maximization (OSEM) method were performed with a Xeleris workstation (GE software version 1.0 M4) with no attenuation or scatter correction. 4DM-SPECT software (revision 1) was used for visual and quantitative analysis of the LV regional perfusion and global ejection fraction (EF). LV regional perfusion was measured in terms of segmental uptake (% uptake), which demonstrates the percentage of the mean pixel count within a particular segment as compared to the maximum segmental mean pixel uptake throughout the LV for summed gated images. LV perfusion was analyzed on a nine segment based pattern, consisting of anterior, anterolateral, lateral, inferolateral, inferior, inferoseptal, anteroseptal, septal and apex regions. All GSPECT and RC-GSPECT reconstructed images were interpreted visually as well as quantitatively by two experienced nuclear medicine physicians who had no access to the clinical data such as selective coronary angiography (SCA) and echocardiography.
Respiratory Tracking
To monitor the respiratory cycle, we used the CT-RPM respiratory gating interface (Varian Medical Systems, Palo Alto, CA). The RPM respiratory tracking system exploits the use of an infrared camera to track a passive marker block placed on the patient. For better understanding of the respiration pattern and optimal localization of the passive marker, the respiration signals of ten volunteer subjects were examined and recorded during a "blank" SPECT study (i.e., without the prior administration of radiopharmaceuticals). A midpoint between the xyphoid process and the umbilicus in the median line of the upper abdomen was determined as the optimal point for setting the passive marker. The system tracks the marker motion to characterize the normal breathing pattern of patients in the form of respiratory waves.
Simultaneous Respiratory and Cardiac Triggering
Each RC-GSPECT study was performed in four steps: a) respiratory tracking by use of the RPM system; b) simultaneous respiratory and cardiac triggering; c) respiratory correction; d) data acquisition and analysis.
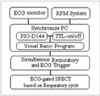
The RPM system and the Varian unit have an X-ray synchronized interface. Since X-ray synchronization is not possible in respiratory ECG gated SPECT acquisition, we changed the Varian output unit to display the respiratory waves on an oscilloscope. A PIO-D144 card, which is transistor-transistor logic (TTL) compatible, was used as an input interface for simultaneous detection of both ECG and respiration signals. The ECG and respiratory cycles were detected by the TTL program on the PIO-D144 input to control the output of the ECG cycles according to the respiratory cycles. If TTL was on low level (on), the ECG cycle was accepted; otherwise, it was rejected (Fig. 1). Therefore, the ECG monitor and the RPM camera were connected to the synchronization computer and the output of this computer was set up for connection to the gamma camera (Fig. 2).
Respiratory Correction
Respiratory correction was performed based on the respiratory motion of patients according to the breathing amplitude. Patients were monitored for a period of one to three minutes to achieve the baseline respiratory pattern as detected by the RPM system (Fig. 3). The RPM system recorded real-time signals, which were synchronized with the breathing motion; therefore, it displayed the respiratory cycle based on both amplitude and phase. This system estimated the inspiration and expiration amplitudes and periods within a respiratory cycle. The end-inspiration (End Insp) and the end-expiration (End Exp) were calculated for ten consecutive respiration cycles for each patient before the beginning of the study. Each respiratory cycle is divided into three bins defined as the average peak interval and irregular peak within the breathing motion of a patient. The End Exp and 2/3 of the End Insp were defined as the lower and upper limits of the accepted respiratory signals, respectively. When the amplitude of the respiratory signal was not within acceptable limits, the cardiac signal was blocked; otherwise, the cardiac signal was transmitted to the acquisition system. This threshold was compatible with the beginning of inspiration and the end of expiration, as illustrated in Figure 1.
Validation of Respiratory Tracking
We used a respiratory phantom and a charge-coupled device (CCD) camera for the evaluation of respiratory phase and amplitude for the validation of the respiratory tracking system. The CCD camera was installed on one end of the SPECT table and the respiratory phantom was placed on the other end, opposing the infrared camera. A marker block was placed on the phantom and patient motion was tracked using a reflected infrared signal from the CCD camera. Block motion was illustrated by the use of RPM software for amplitude and phase within the breath cycles. In this way, appropriate ECG cardiac cycles were selected as acquisition landmarks for each respiratory phase according to the respiratory amplitude and phase.
Statistical Analysis
All data are presented as the mean ± standard deviation (SD). The results of GSPECT and RC-GSPECT were compared by the use of a 2-tailed paired samples t-test. Results were considered significant when the probability value was < 0.05. Pearson's correlation was used to determine the LVEF correlation for the use of GSPECT and RC-GSPECT and echocardiography. All of the statistical analyses were performed by SPSS software package (SPSS, Chicago, IL).
RESULTS
In our patients, the respiratory period in the stress phase was 15% shorter than in the rest phase. This reduction was 10% and 20% for the inspiration and expiration phases, respectively (Table 1). Stress and rest myocardial respiratory motion in the vertical direction was 8.8-16.6 mm (mean, 12.4 ± 2.9 mm) and 7.8-11.8 mm (mean, 9.5 ± 1.6 mm), respectively.
Based on the clinical and scintigraphic findings, 14 out of 26 patients underwent SCA and all of the patients underwent echocardiography within ± 1 week of the test. Nineteen (73.1%) out of 26 patients (9 females, 47.4%; 10 males, 52.6%) showed abnormal myocardial perfusion scans with reversible regional myocardial perfusion defects. Among 15 female patients, nine patients (60%) had abnormal studies and six patients (40%) had normal studies and among 11 male patients, 10 patients (90.9%) showed perfusion defects and one patient (9.1%) had a normal study. The defects were localized in the left anterior descending (LAD) territory in 22 patients, the right coronary artery (RCA) territory in 11 patients and in the left circumflex artery (LCX) territory in 10 patients. For the visual analysis, two reversible perfusion defects in the RCA were detected in two patients only by the use of RC-GSPECT, which were confirmed by the use of SCA. However, the perfusion defects had no consequence for patient management as both of these defects were detected in patients with multi-vessel disease.
According to the SCA findings, three patients had normal coronary arteries and 11 patients demonstrated significant CAD (i.e. > 70% stenosis); four patients had single vessel disease (VD), four patients had two VD and three patients had three VD. Of these patients, three patients had significant stenosis, four patients had non-significant stenosis and seven patients had no stenosis in the LAD artery. Three patients had significant stenosis, five patients had non-significant stenosis and six patients had no stenosis in the RCA. Seven patients had significant stenosis and seven patients had no stenosis in the LCX.
The patient population for the rest study was divided into two groups-one group with a normal RCA (Group 1) and the other group with an abnormal RCA (Group 2). For Group 1, the mean percentage of count density for RC-GSPECT was significantly higher than for GSPECT in the inferior wall (84.98 ± 8.73% versus 78.98 ± 8.83%, respectively; p < 0.001) and the inferoseptal wall (79.73 ± 13.48% versus 76.24 ± 12.76%, respectively; p < 0.001). For Group 2, the mean percentage of count density for RC-GSPECT was significantly higher than for GSPECT in the inferior wall (80.13 ± 10.84% versus 71.93 ± 11.64%, respectively; p < 0.001) and the inferoseptal wall (77.03 ± 15.27% versus 73.98 ± 15.18%, respectively; p < 0.001).
Quantitative assessments of regional perfusion are presented in Table 2 and Figure 4. For the stress and rest studies, the percentage of tracer uptake in the inferior, septal, anteroseptal and inferoseptal walls were significantly higher for the use of RC-GSPECT as compared to the use of GSPECT (p < 0.01). The same results were obtained for the inferior to lateral wall uptake ratio (I/L %uptake) (p < 0.01), which was approximately 6% higher for the use of RC-GSPECT, as is illustrated in Figure 5.
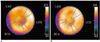
A sample of the GSPECT and RC-GSPECT findings for a rest study derived by the use of polar maps is presented in Figure 6. For the RC-GSPECT polar maps, higher tracer uptake was seen in the inferior wall and particularly in the inferoseptal and anteroseptal walls as comparison to the uptake determined on the GSPECT polar maps.
For the LVEF correlation analysis with the use of GSPECT and RC-GSPECT during a rest study with echocardiography, a better correlation was obtained between the use of RC-GSPECT and echocardiography as compared to the use of GSPECT and echocardiography (y = 0.9654x + 1.6514; r = 0.93, p < 0.001 versus y = 0.8046x + 5.1704; r = 0.89, p < 0.001) (Fig. 7A, B).
DISCUSSION
Cardiac gating assesses both myocardial perfusion and function in a single procedure. This technique is performed with the aid of ECG units. The R-wave is usually chosen for the gating signal as it has the greatest amplitude and is more easily identified in the ECG. Respiratory motion is among the major factors that may affect the quality of MPI and consequently the accuracy of the examination (3, 4). Respiratory motion is a common source of artifacts in MPI studies (8). Respiratory motion is more significant in the vertical versus horizontal direction. The heart moves 9-14 mm towards the apex, and the myocardial walls thicken from approximately 10 mm to over 15 mm between enddiastole and end-systole (23). Accordingly, in view of the intrinsic resolution of current scanners, cardiac motion can lead to significant blurring of the images. The effective image resolution is influenced not only by the intrinsic resolution but also by the full width at half maximum (FWHM) of the distribution of motion. In our study, the range of breathing motion was 8.8 mm to 16.6 mm and 7.8 mm to 11.8 mm in the vertical direction for the stress and rest phases, respectively. This result correlates well with previous reported values (5, 8). In this study, we proposed a new approach for respiratory motion correction to eliminate the effects of respiratory motion in MPI studies.
The use of RC-GSPECT seems to be a more feasible method to assess respiratory as well as cardiac cycles simultaneously. Additionally, the results of our study indicate higher segmental uptake with the use of RCGSPECT as compared to the use of GSPECT, particularly for the inferior wall and septum.
Respiratory gating showed promising results in the elimination of respiratory induced blurring as seen in the myocardial SPECT images (3, 5, 7, 8, 14). Respiratory-gated acquisition requires a sensor to record respiratory motion. Several devices have been introduced for the detection of respiratory motion. These devices include a pressure-based air bag system like a spirometer (17), electrode-impedance plethysmography (14), a mask or nasal canula with a thermal sensor (13) a mouthpiece with a respiratory flowmeter (16), a belt containing a displacement transducer placed around the upper abdomen (15, 18) and the Polaris system with a capability to track respiratory motion for the SPECT imaging system (20). The RPM system, which has been used for respiratory-cardiac gating in PET and radiotherapy, monitors the motion of the chest wall vertically via infrared tracking by means of two reflective markers mounted on a plastic block (21, 22). This system has been widely developed in simulation radiotherapy for tumor tracking of lung cancers (10), CT simulation (12) and PET-CT respiratory-cardiac gating (24). This study is among the first clinical trials that have used the RPM system for respiratory motion tracking in MPI. The advantages of the RPM system are a) recording a real-time image that is synchronized with the breathing motion, b) displaying the respiratory cycle based on both amplitude and phase, c) estimating respiration period with divided inspiration and expiration time analysis and d) each phase of the respiration cycle can be easily analyzed by the user.
In the present study, the acquisition time was identical (i.e. 50 seconds per projection) both with the use of GSPECT as well as with the use of RC-GSPECT. For the RC-GSPECT investigations, ECG signals were not allowed to transmit to the acquisition system while the maximum respiratory amplitude was detected by the RPM system and only if the maximum respiratory amplitude was out of the defined ranged. Hence, the time was kept by the acquisition timer to provide constant acquisition time in both studies, which was about 14 to 19 minutes and depended on the breathing threshold of the patients as well as the ECG cycles.
RC-GSPECT was performed following the GSPECT studies, which may suppose lower counts statistic of this acquisition. Nevertheless, the biokinetic data obtained with the use of 99mTc-Tetrofosmin indicated insignificant changes in myocardial distribution up to 180 minutes post injection (25) and may not significantly affect the counts statistics of the RC-GSPECT studies.
Diaphragmatic attenuation has been suggested as one of the eliminating factors of the image quality in inferior and inferoseptal MPI studies, especially in men. Some clinical studies have recommended the use of an additional prone-positioned SPECT acquisition as well as left lateral planar acquisition in the right lateral decubitus position to overcome this limitation. However, the use of prone position SPECT by itself showed disadvantages due to the requirement for additional imaging as well as the acquisition time (26). The results of this study showed a higher percentage of tracer uptake in the inferior and inferoseptal walls in the RC-GSPECT studies as compared with the GSPECT studies; these findings suggest, that the use of RC-GSPECT may overcome the above mentioned limitations due to diaphragmatic attenuation.
A number of previous studies have used the list mode acquisition technique for respiratory correction in MPI (5, 8, 20). With this method, sorting of the data into gated frames can be performed after acquisition with the use of state-of-the-art scanners with list-mode acquisition capability, whereas ECG-triggered acquisition is employed with only histogram-mode acquisition in conventional scanners. The list mode approach has shown satisfactory results in the elimination of the blurring of the cardiac images; however, it can render a noisier image as compared to a non-gated image. Moreover, list mode acquisition requires substantially more memory and more post acquisition processing than standard acquisition, which may limit its application in routine clinical studies.







 XML Download
XML Download