

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Diagnostic radiology is increasingly used in the assessment and treatment of neonates requiring intensive care. It is often necessary to perform a large number of radiographic examinations that depend on the birth weight of the infant, gestational age and medical problems (1). The age at which exposure takes place is critical in the determination of radiation risk. During fetal development and early childhood, intense tissue proliferation and differentiation takes place, and it is known that proliferating cells are more susceptible to the induction of cancer (2). Radiographic examinations of neonates are particularly critical because of delayed radiogenic cancers as a consequence of a relative longer life expectancy. The small size of neonates, especially of premature infants, places all organs within the useful beam, resulting in a higher effective dose per radiograph than may be the case with older children and adults. Therefore, radiation doses for neonatal X-ray examinations should be kept to a minimum. It is a common practice to keep infants in large rooms together in most neonatal intensive care units (NICU). Our NICU is designed with four incubators present in one room and initially no specific precaution is taken for other infants while a radiographic examination is performed on one of the patients. It is also important to ensure that radiation doses from repeated radiographic examinations carried out frequently in the same room of the NICU should be kept at a minimum. The aim of this work was to determine the radiation doses received by the infants from radiographic exposure and also the contribution from scatter radiation due to radiographic exposure of other infants in the same room.
MATERIALS AND METHODS
Population
A total of 23 neonates with a gestational age as low as 28 weeks and a mean body weight of 1,500 grams were included in the study. The mean duration of hospitalization of the infants was 50 days (range, 6-112 days). The most common requested radiographic examinations for the infant chest and abdomen were used in this study.
Radiographic Technique
All radiographic examinations were performed on one GE AMX-4 and two GE VMX+ mobile X-ray units (GE Medical Systems, Milwaukee, WI). The measured half value layers of these X-ray systems at 50 kVp were 2.24, 2.17 and 2.15 (mm Al), respectively. Performance tests of this equipment (such as accuracy kVp and collimation settings and tube output) were carried out according to the protocols given by the Institute of Physics and Engineering in Medicine (IPEM) (3). Radiographs were acquired using Kodak T-mat G/RA film and Kodak Lanex Regular Screen combination (Kodak Health Imaging, Eastman Kodak, Rochester, NY) with a 400 relative film-screen combination speed. Most examinations were carried out with the baby in an incubator and placed directly on top of the cassette, with a focus-to-film distance of 100 cm. However, some examinations were performed with the baby in a radiant warmer and the distance between the focus-to-film was measured and recorded. Radcal ion chambers (Model 9010 Radiation Monitor Controller, 90 × 6-6 and 90 × 6-180 ionization chambers, MDH Radcal Monrovia, CA) were used for tube output and scatter radiation measurements, respectively. The tube outputs were measured over a range of tube voltages (kVp). A focus to film distance (FFD) of 100 cm was chosen for these measurements.
In order to evaluate the contribution of the scatter radiation, a 5 cm Perspex phantom to simulate an infant was irradiated with the exposure parameters typical for clinical examinations. Since the distance between the NICUs was approximately 2 m, scattered radiation was measured at the NICU level at this distance.
Radiographic Dose Evaluation
Entrance skin doses (ESDs) were calculated from the tube output measurements of the X-ray units in accordance with the following formula:

where the ISL factor is an inverse-square law correction from the focus-to-chamber distance (100 cm) to the focus-to-skin distance (FSD), mAs is the product of tube current (mA) and exposure time(s) used in the infants studies. BSF is the backscatter factor and is taken as 1.1 for the 50-70 kVp range used for a neonate with a body thickness of 5 cm (4). The factor is an inverse-square law correction from the focus-to-chamber distance to FSD, and  is the mass energy absorption coefficient ratio of tissue to air. The mass energy absorption coefficient ratio is equal to 1.05 for the kVp range used in this study (5).
is the mass energy absorption coefficient ratio of tissue to air. The mass energy absorption coefficient ratio is equal to 1.05 for the kVp range used in this study (5).
is the mass energy absorption coefficient ratio of tissue to air. The mass energy absorption coefficient ratio is equal to 1.05 for the kVp range used in this study (5).Lithium fluoride thermoluminescent dosimeter (TLD) chips (3.7 × 3.7 × 0.9 mm) (Model 100: Harshaw Chemical, Solon, OH) in plastic handling pockets (3 for each) were used to measure the total entrance skin dose for both chest and abdomen radiographs for 16 infants, and a Model 3500 Reader (Harshaw Chemical) was used for TLD readout. These pockets were attached to a single point on the skin of a patient for each examination and a pediatrician for each examination determined these locations. In order to minimize batch-to-batch variability, a preselected group of TLDs was calibrated initially and variations of the sensitivities were kept within ± 5%. Calibration of TLDs was carried out for radiographic system using the same X-ray beam qualities as with the neonate studies. A Radcal ion chamber was taken as a reference chamber, and the manufacturer recommendations were considered for these calibrations. A linear regression analysis with the least squares method was used to determine the correlation between ESDTO and ESDTLD. Background radiation was also measured by the use of TLD chips placed outside the radiographic room over the hospitalization time for each infant. Then these values were subtracted from each infant TLD that was used for infant ESD measurements. Effective doses (ED) for each examination were calculated from ESDTO and Monte Carlo conversion factors given from PCXMC software (STUK Helsinki, Finland) (6).
Estimates of radiation risk can be made from the ED. The major risk of concern for an irradiated neonate is childhood cancer. Since most of the neonates in an NICU will be pre-term, fetal risk factors for estimating the risk of a childhood cancer following neonatal exposure were used for the neonate risk calculations (7).
RESULTS
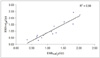
The mean numbers of radiographs received by one infant were 14 and 5 for chest and abdomen examinations, respectively. The mean ESDTO per radiograph was calculated by dividing the sum of the ESDTO by the total radiography numbers for each examination. The mean ESDTO per radiograph were 67 µGy and 65 µGy for the chest and abdomen, respectively. The mean ESDTLD was 70 µGy. ESDTLD was well correlated with ESDTO obtained from the total chest and abdomen radiographs for each infant (R2 = 0.86) (Fig. 1).
The measured scattered radiation range at a 2 m distance from the NICU was 11-17 µGy per radiograph. Considering the mean ESD as 65 µGy per radiograph, the contribution of the scatter radiation is negligible. The radiation dose of an infant received from the scatter radiation from the irradiation of other infants is approximately 1/4,600 times the direct exposure of the infant. Table 1 summarizes the radiographic data, ESDTO and ED for each examination accrued in this study.
Using the overall risk factors for inducing a fatal childhood cancer in the first decade of life following prenatal radiation exposure based on ICRP60 (2.8 × 10-2 Sv-1 to 13 × 10-2 Sv-1) yields somatic risk estimates of 0.4 × 10-6 to 2 × 10-6 and 0.6 × 10-6 to 2.9 × 10-6 for chest and abdomen radiographs, respectively (7).
DISCUSSION
The ESDs were comparable to the mean values reported by the Commission of European Communities (EC) as 80 µGy (8) and by the National Radiological Protection Board (NRPB) as 50 µGy for chest radiographs (9). Exposure of infants to radiation in the vicinity of the exposed infants in the same room is very low, practically for the range of the lowest detectable dose.
The difference between ESDTLD and ESDTO may be attributable to variations on the tube outputs and errors of the focus-to-skin distance measurements. The ESD values per radiograph were found to be higher than the values reported in the literature (1, 4). The use of low tube potential (kVp) values in this study probably is the reason for higher doses. According to Duggan et al. (10), increasing the tube potential from 50 kVp to 60 kVp reduced ESD by 9%. Table 2 shows a comparison between exposure parameters, ESDTO, ED and risk factors for childhood cancer per examination for this study and other studies.
This is the first dosimetry study performed for an NICU in Turkey and we measured radiation near the exposed infant in the same room to check safe distances in the NICU for scatter radiation. If the high kV technique had been used in this study, the doses delivered to patients could have been substantially reduced. There is a continuing need for assessment of radiation dose in the neonate healthcare centers along with a regular review of dose reduction procedures. The results obtained from this study show that the ESDTLD and ESDTO indicated no significant differences.
Because of their sizes, a relatively large area of the infants was irradiated and it was more difficult to shield radiosensitive organs. In addition, measurement of infant dose must be performed in sterile conditions as soon as possible because of the high sensitivity of the infants to infection.
The results of our study show that neonates received acceptable doses from common radiological examinations. Although the contribution of scatter radiation to the neonatal dose is low, considering the sensitivity of the neonates to radiation, further protective action should be performed by increasing the distance between patients until the effect of scatter radiation disappears.


 XML Download
XML Download