

 PDF
PDF ePub
ePub Citation
Citation Print
Print


The recent development of multi-detector computed tomography (MDCT) scanners allow for the exact quantification of peripheral airway geometry, which in turn provide important information for evaluating regional airway physiology and structure. In particular, the elucidation of bronchial tree dimensions can be used to evaluate and track the development of diseases affecting the airways, such as asthma and chronic obstructive lung diseases, as well as to determine the efficacy of new therapeutic approaches (1, 2). To date, such studies have for the most part, been limited the assessment of airway dimensions into the airways perpendicular to their local long axis in order to avoid the overestimation of pleural wall thickness or luminal diameters associated with the oblique sectioning of a tubular structure (3-7). It is especially important to accurately measure an oblique airway, since most peripheral airways are tilted in the axial section. Only a few researchers have measured the airway as a result of this airway obliquity. Saba et al. studied oblique airway measurements using a physical phantom and an elliptical fitting (8). However, this method assumed that the airway lumen is circular.
In addition, there is a large estimation error in the tilt angle in the case of a small airway, due to the partial volume effect. For a virtual bronchoscopy, several studies have addressed the detection of the airway center line (9, 10). However, these studies do not focus on the accurate measurement of the tilted airway dimension to the axial scan plane, but rather on the accurate path generation of the camera.
The aim of this study was to develop an algorithm which accurately measures the dimensions of an obliquely oriented airway to an axial scanning plane assessed by volumetric CT, and to evaluate the degree of influence on the measurement accuracy of the obliquity of an airway and the interacting factors including, which include the CT imaging parameters and airway sizes, using the full width at half maximum (FWHM) method. In addition, we attempted to create a clinically viable recommendation for oblique airway measurement using the FWHM method.
MATERIALS AND METHODS
Airway Phantom and Measurement
A phantom was composed of eleven poly-acryl tubes which simulated airways of various inner diameters and wall thicknesses, ranging from 1.26 to 8.46 mm and from 0.45 to 3.08 mm, respectively. The details of the airway phantom design and measurement have been described in our previous report (11).
CT Scan and Data Storage
The phantom was scanned at various tilt angles (i.e., 0, 30, 45, and 60°), to the axial plane on a 16-multi-detectorrow CT scanner (Siemens Sensation 16, Siemens Medical Solutions, Erlangen, Germany). The CT scan parameters included a 16 × 0.75 mm collimator with 100 effective mAs, a pitch of 1.0 and 120 kVp, a 512 × 512 matrix setting, and a 360-mm field of view (FOV). The CT images were reconstructed using every combination of the following parameters: five different reconstruction kernels (B10f, B30f, B50f, B70f and B80f); tilt angles (0, 30, 45, and 60°) to the axial plane; and slice thicknesses (0.75, 1, and 2 mm) (Fig. 1). A reconstruction kernel of B10f corresponds to a soft reconstruction kernel, as opposed to B50f, which is standard, and B80f, which is a sharp reconstruction kernel. The resulting 2D image data were stored in the Digital Imaging and Communications in Medicine (DICOM) format.
Data Processing and Analysis Procedure
In-house software was developed at the Asan Medical Center to accurately measure airway wall thickness and luminal radius. Figure 2 shows the schematic diagram of the data processing and analysis. In addition to the data process steps described in our previous report, we added two steps for axis determination of an oblique airway and for image reconstruction perpendicular to the axis (Fig. 2).
Estimation of the Medial Axis of Oblique Airways
The medial axis of oblique airways was estimated using a 3D distance map. A 3D distance map is the simplest and the most convenient way to represent and store the set of points furthest from the airway boundary. Moreover, a 3D distance map is a three-dimensional array where the x, y, and z distance information corresponds to the rows, columns, and depths, respectively. An example this is CT volume data and the corresponding distance from the boundary (distance values) are stored in the array's elements (pixels). The 3D distance map is like a grey scale image except that the distance information (float - 32 bytes) replaces the intensity information. In addition, after generating a 3D distance map, the centroid of the upper and lower slices along the medial axis of the oblique airway was re-calculated to obtain a more accurate estimated axis of the airway.
Measurements and Statistics
After image reconstruction of every combination of tilt angle and reconstruction parameters (axis, wall thickness, and luminal radius) of each artificial airway, the CT images were measured using the in-house software. Each measurement was performed ten times at different medial axes, and the average numbers were used for statistical analysis.
To assess the effectiveness of axis determination, the actual angle of each tube, and the estimated angle of the CT images of the physical phantom were compared using a Student's t-test. To determine the effects of the orientation of the airway, the actual and measured dimension of each tube from the various oblique CT scans were compared using a repeated ANOVA test. The accuracy of the actual and estimated measurements was evaluated using the Bland-Altman method. The paired t-test was used to determine the possible presence of a significant difference between each set of measurements and the reference of the actual dimension. A p value less than 0.05 was considered a statistically significant difference. The t-test for single means was performed using StatisticaTM 7.0 (StatSoft, Tulsa, OK).
RESULTS
Axis Estimation
The axis estimation method using a 3D thinning algorithm was evaluated on CT scans at various tilt angles (0, 30, 45, and 60°), a 0.75 mm slice thickness, and a standard reconstruction kernel (B50f). All eleven poly-acryl tubes were evaluated and compared. The mean error and standard deviation (SD) of each tilt angle were 0.0 ± 0.0° at 0°, 30.51 ± 1.57° at 30°, 44.97 ± 1.10° at 45°, and 59.91 ± 0.96° at a 60° tilt angle. The overall absolute error of the medial axis estimation were 0.0 ± 0.0° at 0°, 1.35 ± 0.85° at 30°, 0.62 ± 0.88° at 45°, and 0.74 ± 0.56° at a 60° tilt angle. The estimated tilt angles were not significantly different from the actual tilt angles (t-test for single samples) (Table 1).
Airway Wall Thickness
Effects of Obliquity and Estimated Wall Thickness
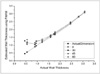
Figure 3 shows the actual and estimated wall thicknesses of the airway at the four measured tilt angles. We found no statistically significant difference among the four tilt angles with 0.75 mm slice thickness, a standard reconstruction kernel (B50f), and an FOV of 360 mm, although general increases in measurement error increased as the tilt angle increased from 0° to 60° (Table 2). If the wall thickness of the airway is less than 1 mm and therefore be within the magnitude of a single pixel, a rapidly increasing amount of errors was observed in the airway wall measurement. The small airway with less than a 1-mm wall thickness (1st and 2nd airways) were excluded in all of the statistical tests performed to determine the degree of error.
Effects of Obliquity and Slice Thickness
As the image thickness increased and a larger tilt angle of airway axis was used, the estimated wall thickness became smaller than the actual wall thickness (Fig. 4). There was an internal interaction between the slice thickness image parameters and the obliquity of the airway on the measurement accuracy which demonstrated a statistically significant difference among the tilt angles (p < 0.001). The measurement of the CT image with a thickness of 0.75-mm resulted in the most accurate and independent measurement of the obliquity of an airway, which was not statistically different from the actual wall thickness.
Effects of Obliquity and the Reconstruction Kernel
Figure 5 shows the interaction of airway obliquity and the reconstruction kernel on the measurement of airway wall thickness. When a sharper reconstruction kernel was used and the airway was tilted at a larger angle, the estimated wall thickness became smaller than the actual wall thickness (Fig. 5). Moreover, a significant internal interaction (p < 0.001) was observed between the reconstruction kernel and the obliquity of an airway at the different tilt angles. Measurement of the CT images reconstructed by a standard kernel (B50f) resulted in the most accurate measurement, measuring of the obliquity of an airway. With these imaging parameters, there was no significant difference between was observed between the estimated measurement of the airway wall thickness at all tilt angles.
Luminal Radius
Effects of Obliquity and Estimated Luminal Radius
No statistical significant was found in the measurement of the difference between the measured luminal radii and actual radii among the four tilt angles when using a slice thickness of 0.75 mm, standard reconstruction kernel (B50f); and FOV at 360 mm, although there were general increases in measurement error as the tilt angle increased from 0° to 60° (Table 3).
Effects of Obliquity and Slice Thickness
As the image thickness increased and a larger tilt angle of airway axis was used, the estimated radius became smaller than the actual radius (Fig. 6). A statistically significant internal interaction between the slice thickness image parameters and the obliquity of the airway on the measurement accuracy was observed at the different tilt angles (p < 0.001). The measurement on the CT image at a 0.75-mm thickness resulted in the most accurate measurement, independent of the obliquity of an airway, which was not significantly different from the actual luminal radius.
Effects of Obliquity and Reconstruction Kernel
Figure 7 shows the interaction between the airway obliquity and the reconstruction kernel in the measurement of the airway luminal radius. When a sharper reconstruction kernel was used and the airway was tilted to a larger angle, the estimated radius became smaller than the actual radius (Fig. 5). A statistically significant internal interaction between the reconstruction kernel and the obliquity of an airway was observed at the different the tilt angles (p < 0.001). The measurement of the luminal radius was independent of the airway obliquity. The standard kernel (B50f) yielded the most accurate results.
DISCUSSION
To accurately measure the airway dimension when the airway is oriented obliquely, it is essential to generate an image perpendicular to the airway axis. Our phantom study has shown that accurate axis determination of an obliquely oriented airway is possible using the proposed algorithm at a 60° tilt angle.
This study also demonstrated that there exists a complex interaction between the airway obliquity and the various CT scan parameters in the determination of airway measurement accuracy. Slice thickness and reconstruction kernel factors interacted significantly with tilt angles. In our study, the decrease in accuracy of measurement was proportional to the increase in slice thickness in the measurements of airway wall thickness and luminal radius. This result is expected when considering the partial volume effect. At a 0.75-mm slice thickness, the accuracy of measurement is guaranteed at tilt angles of 0 to 60 degrees. As the FOV of this study is 360 mm, the Z-axis resolution of 0.75 mm results in an approximately isocubic voxel resolution. In the case of a reconstruction kernel, the standard kernel (B50f) offered the best accuracy. By combining a 0.75-mm thickness and a standard reconstruction kernel, we were able to reliably measure the dimension of the tubes regardless of their oblique orientation. Similar to the results of the previous study, the CT scans with various tilt angles also showed that there is a threshold which rapidly increases the error of the airway wall measurement when using the FWHM method with a wall thickness less than 1 mm. This result suggests that with current commercial instruments, it is possible to correctly measure the dimension of airways located obliquely to the image plane when the images are reconstructed at a sub-millimeter slice thickness and a standard reconstruction kernel, although a clear limitation exists in the measurement of airways smaller than 1 mm in wall thickness.
Future studies should evaluate the measures necessary for the clinical application of the correct airway wall measurement at airway wall thicknesses below 1 mm. Even though the measurement using the FWHM method with a wall thickness less than 1 mm was not correct, the magnitude of the CT profile is proportional to wall thicknesses below 1 mm. Consequently, a modified FWHM may need to be developed.
In conclusion, we verified that the accurate determination of the airway axis located in the oblique direction on a volumetric CT is feasible using the proposed algorithm. There are strong significant interactions in the measurement accuracy between airway obliquity and the CT parameters. For a clinically acceptable measurement of airway thickness without considering obliquity, we recommend obtaining CT images at a sub-millimeter slice thickness and a standard reconstruction kernel.









 XML Download
XML Download