

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Abbreviations
AC-PC
anterior commissure-posterior commissure
CP
cerebral peduncle
CSTs
corticospinal tracts
DTI
diffusion tensor MR imaging
EPI
echo-planar imaging
FA
fractional anistropy
MPRAGE
magnetization-prepared rapid-acquisition gradient-echo
PCG
precentral gyrus
PLIC
posterior limb of the internal capsule
ROI
region of interest
Diffusion tensor MR imaging (DTI) and tractography (DTT) can depict white matter tracts of the brain in vivo. Recent DTT studies have demonstrated relatively unanimous results regarding the location of the corticospinal tract (CST) in the posterior limb of the internal capsule (PLIC) and the brain stem as determined by the use of DTI (1-4). However, controversy remains about the somatotopic organization of the pyramidal tract at PLIC. A recent DTT study demonstrated the somatotopic organization of the CST in the PLIC, in which the hand fibers were located anterolateral to the foot fibers, and the somatotopic organization showed transverse orientation at the PLIC (1). Additional DTT studies showed results suggesting an anteroposterior orientation of the pyramidal fibers at the PLIC (4, 5). Until now, there have been no remarkable DTT results about the organization of the pyramidal tract at the cerebral peduncle (CP). The goal of this study is to evaluate the somatotopic organization of the CSTs in the PLIC and CP, and to demonstrate the relationship of the organization among the precentral gyrus (PCG), PLIC, and CP by the use of DTT.
MATERIALS AND METHODS
We imaged the brains of nine healthy right-handed subjects. Four male and five female volunteers (mean age: 34 ± 5.4 years) were included in the study and all had normal results on physical and neurological examinations. Informed consent was obtained from all the subjects after the nature of the MR examination had been fully explained.
The DTI data was obtained with a 1.5 T MR unit (Magnetom Sonata, Siemens Medical Solutions, Erlangen, Germany). We used a spin-echo EPI sequence with 12 diffusion-sensitized directions (TR/TE = 5300/100 msec, number of excitations = 3, b-value = 0, 1000 s/mm2, field of view = 24 cm, 128 × 128 matrix, 3 mm thickness with no gap, parallel to anterior commissure-posterior commissure (AC-PC) line, covering from the pons to the high convexity). We also obtained anatomical T1 and T2-weighted images and magnetization-prepared rapid-acquisition gradient-echo (MPRAGE) images, which were correlated with the DTI images. The DTI map and tractography were calculated using DTI task card version 1.7 (Magnetic Resonance Center, Massachusetts General Hospital, Boston, MA) on a Siemens scanner. An angular threshold of 35 degrees and a fractional anistropy (FA) threshold of 0.25 were used. We defined the CSTs by using a two region of interest (ROI) approach. The first ROI was placed on the left side of the pons, which was an expected area for a CST on the DTI color map (Fig. 1A). The second ROI was placed on the left side of the lateral half of the PLIC (Fig. 1B). The fiber tracts crossing these two ROIs and the PCG, which was identified by using known anatomic landmarks such as the cerebral sulci, including the superior frontal, precentral and central sulci, and the omega shaped posterior knob (6, 7), were defined as CSTs (Fig. 1C). Four new ROIs were then drawn at the PCG from the medial to lateral direction as ROI 1 (most medial) to ROI 4 (most lateral) (Fig. 1D). Finally, we defined each fiber tract of the CSTs between the pons and each ROI in the PCG by using two ROIs methods. The tractography results were assigned a different color for the each of the CSTs from the medial to lateral direction (ROI 1-pink, ROI 2-blue, ROI 3-yellow, ROI 4-red). The location and somatotopic organization of the CSTs at the level of the CP and PLIC were evaluated by using multiple projection views. The reconstruction time for tractography was less than twenty minutes per each subject.
We initially drew an ROI for the CST of the whole PLIC, but some fibers descended posterior to the CP, near to the medial lemniscus.
By using two ROI methods, we could not find any fiber tracts between the pons ROI and the medial half of the PLIC. By single ROI tracking at the medial PLIC, the fiber tracts from the medial half of the PLIC descended near to the medial lemniscus of the midbrain and they never traversed the CP, but they ascended to the medial portion of the PCG, supplementary motor area, and to the postcentral gyrus area (Fig. 2).
RESULTS
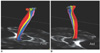
In all cases, the two medial ROIs (ROI 1 and ROI 2) were located slightly posterior to the two lateral ROIs (ROI 3 and ROI 4) at the PCG. In the all subjects, the CSTs traversed the mid to posterior portion of the lateral half of the PLIC, and showed somatotopic organization along the long axis (anterior-posterior) of the PLIC. The CSTs from ROI 1 and ROI 2 (foot fibers) were located posterior and medial to the CSTs from ROI 3 and ROI 4 (hand fibers) in the PLIC (Fig. 3). In all subjects, the CSTs traversed the mid to lateral portion of the CP, and they showed a transverse orientation (right to left) of the somatotopic organization in the CP. In the left hemisphere, the CSTs looked like they were rotating in a clockwise direction descending from the PCG to the CP and the foot fibers were located lateral to the hand fibers in the CP (Fig. 4). In four cases, intermixing of the fibers was present within the hand fibers. The CSTs from ROI 3 were divided as anterior and posterior bundles, and the CSTs from ROI 4 were located between the anterior and posterior bundles of ROI 3 at the PLIC and the CP (Fig. 5).
DISCUSSION
Despite of the limited spatial resolution of DTT for the tracking of human axonal fibers, two recent DTT studies have described the somatotopic organization of the CSTs and sensory tracts (1, 5). There is controversy concerning these two studies about the somatotopic organization of the CSTs. In one study, the hand-foot fibers were organized along the short axis of the PLIC like the hand-foot homunculus in the PCG, and rotation of pyramidal tract was not mentioned (1). In the other study, the hand-foot fibers were organized along the long axis of the PLIC and had an approximate 90° rotation as they descended from the PCG (5). Our DTT results were similar with the latter study and showed antero-posterior alignment of the CSTs and a clockwise rotation descending from the PCG to the CP in the left hemisphere. Recent clinical symptoms based studies also support the antero-posterior orientation of the somatotopic organization of the CSTs in the PLIC (4, 8). In these two studies, a more anterior located lacunar infarction in the PLIC and corona radiata was correlated with symptoms of the face and arm.
The CP of the midbrain, where the CSTs are densely concentrated, was less sensitive to a susceptibility artifact of DTI and DTT may reliably visualize white matter tracts. The CSTs were located at the mid to lateral portion of the CP, according to previous DTT studies (2, 9). Our DTT results also showed a similar location of the CSTs at the CP. There have been no DTT reports about the somatotopic organization of the pyramidal tracts at the midbrain level. The CSTs were organized along the horizontal (mediolateral) direction at the CP in our study. The CSTs had about an 180° rotation as they descended from the PCG, and the hand fibers were located medial to the foot fibers.
We drew only the lateral half of the PLIC for tracking of the CSTs as the fiber tracts made by tracking a single ROI from the medial half of the PLIC did not go through the CP in the midbrain. In previous DTT reports, it was noted that the PLIC contains part of the thalamocortical pathway (3, 10). These thalamic radiations included pathways between the ventrolateral, ventral anterior, ventral posterior nuclei of the thalamus and premotor, and the motor cortex (10). In our study, the fiber tracts from the medial half of the PLIC showed a similar course of these thalamic radiations, thus we considered the fiber tracts from the medial PLIC as part of thalamic radiations. In our opinion, it is better to select one of the seed ROIs at only the lateral half of the PLIC for determining accurate tractography of the CSTs.
We used DTT software based on the streamline methods in our study; so an inherent limitation for the tracking of crossing fibers within a voxel was present (11, 12). The fiber tracts evaluated in the present study included only the fibers from the hand, trunk and leg area of the PCG due to this limitation of the DTT method (5, 13). Our study showed intermixing of some fibers within the CSTs as in a previous study (1). However, there has been no anatomic specimen based study describing intermixed fibers within the CSTs. This intermixing of fibers may be true or erroneous and we could not exclude the possibility of an error related with the crossing fibers within a voxel.
In conclusion, the CSTs from the anterior PCG ROI (hand fibers) were located anterior in the PLIC and medially in the CP. The CSTs were organized along the long axis of the PLIC and the horizontal (mediolateral) direction at the CP. The orientation of the somatotopic organization of the CSTs was rotated in a clockwise direction descending from the PCG to the CP in the left hemisphere. Knowledge of the exact location, orientation, and organization of CSTs through internal capsule, CP provided in our investigation may help in the performance of delicate functional neurosurgery such as deep brain stimulation and neurosurgery for brain tumors. In addition, the findings are be helpful in understanding the emerging clinical sequelae that present in the motor domain following a localized trauma or a lacunar infarction.




 XML Download
XML Download