

 PDF
PDF ePub
ePub Citation
Citation Print
Print


MRI has been used to evaluate anterior cruciate ligament (ACL) grafts in patients with persistent or recurrent symptoms after reconstruction surgery. Many studies have been concerned with the MR appearances of ACL grafts after reconstruction surgery, and some of them have described the abnormalities of the ACL graft, including graft impingement and tear (1-6). Various MRI techniques have been applied to determine which image offers optimal ACL graft visualization. The majority of these MR studies have evaluated ACL grafts using orthogonal sagittal and coronal images with or without the oblique sagittal images. Only a few studies have used the oblique axial or oblique coronal images for assessing ACL grafts (7-9).
The additional use of oblique coronal imaging improves the diagnostic accuracy in terms of grading native ACL injuries (10-12). However, to the best of our knowledge, no previous study has assessed the diagnostic value of oblique coronal imaging for evaluating ACL grafts. We hypothesized that including the oblique coronal MR images into the routine knee MRI will be helpful in assessing the status of a ACL graft after ligament reconstruction surgery. The purpose of this study was to determine the diagnostic benefit of additional oblique coronal MRI for evaluating ACL grafts.
MATERIALS AND METHODS
Approval from our institutional review board was obtained for this retrospective study. At our institution, the patients with a history of ACL reconstruction surgery undergo MRI when they have persistent, recurrent or new symptoms or they have re-injured their knee. After clinical examination and reviewing the MR images, follow-up arthroscopic examinations were performed for patients suspected of having a torn ACL graft or other internal derangement of the knee. A computer search of the MRI examinations that were done at our hospital from June 2000 to March 2007 yielded 120 consecutive patients who underwent MRI of the knee after ACL reconstruction surgery. Of these patients, 48 had follow-up arthroscopic examinations of the knee. Finally, 51 consecutive MR examinations in 48 patients (40 men and 8 women, age range: 18-60 years, mean age: 32 years) were included in this study. The MR examinations were performed at a mean of 31 months (range: 4-192 months) after the initial ACL reconstruction surgery. The mean time interval between the postoperative MR examinations and the follow-up arthroscopy was 50 days (range: 0 day-9 months). All the arthroscopies were performed by two expert orthopedic surgeons. The arthroscopic records revealed 26 cases with intact ACL grafts, 12 with partially torn ACL grafts and 13 with completely torn ACL grafts. The graft materials we used were autogenous quadriceps tendon (n = 39), autogenous bone-patellar tendon-bone (n = 9) and allogenous Achilles tendon (n = 3).
MRI Protocol
MR examinations were performed on 1.0-T or 1.5-T MR scanners (Siemens, Erlangen, Germany). The MRI protocols included the sagittal spin echo T1-, the turbo spin echo T2- and the proton density-weighted images, the coronal turbo spin echo T2- and the proton density weighted images and the oblique coronal turbo spin echo T2-weighted images. The oblique coronal T2-weighted images were obtained in the plane parallel to the course of the femoral intercondylar roof on the sagittal scout images (Fig. 1). The parameters of the routine knee MRI were as follows: TR/TE = 500/12 (T1-weighted image), 3500/15 or 2200/14 (proton density weighted image), 3500/98 or 2200/90 (T2-weighted image), a 4-mm slice thickness, a 0.2-mm interval and a 256×256 or 512×512 matrix. The oblique coronal T2-weighted image parameters were as follows: TR/TE = 3000-4000/96, a 3-mm slice thickness, a 0.15-mm interval, a 256×256 or 512×512 matrix and a 3-minute 8-second or 3-minute 55-second acquisition time.
Imaging Analysis
The images were retrospectively reviewed by two musculoskeletal radiologists with 14 years and nine years of experience, respectively. These readers were blinded to the arthroscopic results. The imaging sequences were grouped into two evaluation sets by a radiologist who was not involved in imaging interpretation. Initially, each reader independently evaluated the status of each ACL graft with using the routine knee MR images only (imaging group A) and then with using the routine knee MR images in combination with the oblique coronal images (imaging group B).
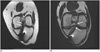
The severity of ACL graft injury was graded using a 3-point system; i.e., grades 0, 1, 2 (1, 4). Grade 0 implied an intact graft, grade 1 a partial tear and grade 2 a complete tear. We regarded an intact graft as a low signal intensity graft with or without longitudinally increased signal intensity streaks, well-preserved continuation and a taut orientation. Some grafts with focal or rarely diffuse increased signal intensity or a slight lax orientation were included as intact grafts (2). On the other hand, hyperintensities were almost equal to fluid or graft thinning in the ACL grafts on the T2-weighted images were considered suggestive of a partial or full thickness graft tear (13, 14). To differentiate grade 1 and 2 injuries, a near full-thickness defect, the lack of continuity or an indistinct ligament contour were considered indicators of grade 2 injury (Fig. 2).
In addition to assessing the severity of graft injury, the two readers were requested to assign a confidence level for the diagnosis in the two imaging groups based on a 5-point scale, that is, 1: completely uncertain, 2: small likelihood, 3: equivocal, 4: probable and 5: very certain.
The arthroscopic reports were reviewed to determine the status of the ACL grafts. The MR results were compared with the arthroscopic reports as reference standards.
Statistical Analysis
Weighted kappa statistics were used to assess the diagnostic agreement between the MRI diagnoses and the arthroscopic results of the two imaging groups (11). Interobserver agreement was also calculated using weighted kappa statistics. The strength of agreement was interpreted according to the guidelines described by Landis and Koch (15), that is, 0: poor, 0.01 - 0.20: slight, 0.21 - 0.40: fair, 0.41 - 0.60: moderate, 0.61 - 0.80: substantial and 0.81 - 1.00: almost perfect.
Confidence levels for interpretation were scored for each imaging group, and the difference in the confidence levels between the two imaging groups was assessed using the paired t-test. The sensitivity, specificity and accuracy for detecting graft tear were calculated by grouping the grade 1 and 2 injuries. A p-value of less than 0.05 was considered statistically significant.
RESULTS
The MR grades of the ACL graft injury for each reader and each imaging group are summarized in Tables 1 and 2, respectively. The diagnostic agreements between the MR grade and the arthroscopic grade for imaging group A were considered "moderate" with weighted kappa values of 0.555 (reader 1) and 0.515 (reader 2). On the other hand, those for imaging group B were "substantial" with weighted kappa values of 0.666 (reader 1) and 0.611 (reader 2). Between the two imaging groups, a mismatch was noted for seven cases (downgrading for 6 and upgrading for 1) by reader 1; there were mismatches for eight cases (downgrading for 5 and upgrading for 3) by reader 2. The readers reached the correct diagnoses in eight cases (5 cases by reader 1 and 3 cases by reader 2) of the 11 cases for which they downgraded an ACL graft injury on the oblique coronal imaging, and the arthroscopic results were seven cases with an intact graft and one case with a partially torn graft (Figs. 3, 4). In three cases (1 case by reader 1 and 2 cases by reader 2) of the four upgraded cases, the correct diagnoses were achieved on the oblique coronal imaging and the arthroscopic results were two cases with a partially torn graft and one case with a completely torn graft.
Interobserver agreement between the two readers was considered "substantial" with weighted kappa values of 0.614 (imaging group A) and 0.730 (imaging group B). The confidence levels for MR evaluation of graft injury are listed in Table 3. The confidence level for imaging group B was significantly higher than that for imaging group A (p < 0.01). The mean confidence level for the correct diagnosis was higher than that of the incorrect diagnosis for each reader and each imaging group (p < 0.01).
The overall MR sensitivity, specificity and accuracy for the diagnosis of ACL graft tear were calculated by combining grade 1 and 2 injuries as tear (Table 4). The imaging of group B had higher specificity and accuracy than did the imaging of group A for each reader.
DISCUSSION
In our study, the diagnostic accuracy for ACL graft injury was improved by the addition of oblique coronal imaging to the routine knee MR sequences. The overall MR specificity and diagnostic accuracy for ACL graft tear were also improved by the addition of the oblique coronal imaging. Oblique coronal imaging may lead MR readers either to downgrade or upgrade the ACL graft injury that is originally seen on routine knee MRI, and so this helps reach a correct diagnosis. The MR readers were more confident of graft assessment with viewing the additional oblique coronal imaging than by viewing the routine knee MRI alone.
Staeubli et al. (16) recommended using the oblique coronal MRI for visualizing the anatomic diagonal course of the native ACL and its relation with the intercondylar notch and the posterior cruciate ligament. For the native ACL, the use of additional oblique coronal images improves the specificity and accuracy for detecting ACL tear and this also raises the accuracy of grading ACL injury (11). For the ACL graft, one previous study included the oblique coronal images for the evaluation of healthy ACL grafts (7).
The reasons why the diagnostic accuracy was enhanced by the additional oblique coronal images in our study are presumed to be as follows. First, the full length of an ACL graft can be viewed in a single plane along its anatomic diagonal course, and thus, the graft is less subject to volume averaging. Second, the transverse width of an ACL graft can be easily appreciated on the oblique coronal images because both the medial and lateral margins of the graft are clearly visualized. Third, the oblique coronal imaging reduces paramagnetic artifacts by avoiding fixation devices in the plane, while the artifacts from metallic fixation screws obscured the femoral and tibial bone tunnels on orthogonal sagittal and coronal images.
Many studies have described the MR appearance of ACL grafts after reconstruction surgery. The majority of the previous MR studies have employed sagittal, coronal or oblique sagittal images (1-6, 17). Some investigators have conducted MR studies using proper knee positioning in order to optimize visualization of an ACL graft (18). Contrast-enhanced MR studies have been performed to evaluate the periligamentous tissue with its higher signal intensity, and this higher signal intensity was derived from neovascularization, granulation tissue or immature collagen (19-21). Two previous studies evaluated the oblique axial images obtained at a right angle to the ACL graft (8, 9), and one report used MR arthrography for ACL graft assessment (22). These studies have shown various accuracies for conventional MRI; the largest of these studies on 52 patients, and two of these 52 patients had torn grafts, showed 100% sensitivity, 86% specificity and 86.5% accuracy for detecting a tear (17).
The diagnosis of partial tear of an ACL graft is more difficult than that of complete tear: on a conventional MR study of 16 patents, the diagnosis of partial tear versus other conditions (intact graft or complete tear) resulted in 0% sensitivity, 67% specificity and 37.5% accuracy (1). Similar in our study, false positive or negative diagnoses of partial tear were the main causes of the relatively low accuracy for the overall grading of ACL graft injury on MRI. The readers found it difficult to correctly ascertain a normal or partially torn graft when a subtle abnormality was suspected within the graft on MR images. Using the oblique coronal images reduced the false-positive diagnosis of partial tear and increased the specificity of MRI for ACL graft injury. Nevertheless, false negative diagnoses for ACL graft injury were still made with using the oblique coronal images. We believe that the femoral attachment site is vulnerable to misinterpretation because of the acute angle formed between the femoral tunnel and the grafts on the oblique coronal images. The oblique sagittal images may help improve the visualization of the femoral attachment site of an ACL graft by showing the femoral tunnel in a plane (2). In other cases, a slightly attenuated, lax ACL graft at arthroscopy had a normal appearance on MR images. The readers made many false negative diagnoses even with using the oblique coronal images because the MR diagnoses were based on the morphologic abnormalities, and there was insufficient information on such functional abnormalities as graft laxity. For these cases, we may reduce the rate of a false negative MR diagnosis by referring to the clinical data.
Some limitations of the current study should be mentioned. First, our study population included only a small number of patients with partial or complete ACL graft tears. Second, the time interval between the MR examination and arthroscopy, as well as the chronicity of graft tear, which might have affected the MR findings, were disregarded in our study. Third, because the weighted kappa statistic does not provide a p value, we could not calculate the statistical significance of the difference between the diagnostic accuracies of the two imaging groups.
In conclusion, our results suggest that the use of additional oblique coronal images improves both the diagnostic accuracy and the diagnostic confidence for grading ACL graft injury. Using the oblique coronal images also increases the specificity and accuracy of ACL graft tear, and this may help physicians make correct clinical/surgical decisions when treating these ligament injuries.







 XML Download
XML Download