

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Hydatid disease (HD) is a parasitic disease that's most commonly caused by the larval stage of Echinococcus granulosus. It is still a considerable health problem in the world (1). E. granulosus can reach any organ or tissue in the body where it develops into small hydatid cysts (1-5). The wall of the cyst contains three layers. The outermost layer is the pericyst, the middle layer is the laminated membrane and the innermost layer is the germinal epithelium (endocyst) (1-3, 5). The latter is the only living part of the hydatid cyst and it produces the laminated membrane and infectious scolices that represent the larval stage of the parasite (5). The characteristic imaging findings have been described as calcification of the cyst wall, the presence of daughter cysts and membrane detachment (3). However, the radiological signs are usually non-specific. Serologic tests may be helpful in the diagnosis, but their reliability is not 100% (5). Unusual sites of this disease can frequently cause diagnostic problems and so this can give rise to an increased risk of diagnostic delay and many potentially serious complications. Even a mortality rate of 4% for this disease was reported in the literature (6, 7). In this paper, we describe the radiologic findings of HD in some uncommon sites besides the liver and lung, as based on our experiences.
RADIOLOGIC FINDINGS
A pathology-based classification for this disease has been described by Lewall (1). The early lesions (type I hydatid cysts [HCs]) have a non-specific anechoic cystic appearance on ultrasonography (US) (1-4). On CT scans, Type I HC appears as a well-defined, round or oval cystic mass with an attenuation density near that of water (3-30 HU) (Fig. 1). On magnetic resonance imaging (MRI), HC is seen as hypointense on T1-weighted images and as marked hyperintense lesions on T2-weighted images. MRI can displays a low-signal-intensity rim that surrounds the cyst (the "rim sign"), which is more evident on the T2-weighted sequences (2, 8).
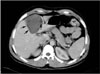
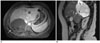
For type II HCs, many daughter cysts and/or matrix develop within the parent cyst with or without cyst wall calcification (Fig. 2) (1). Daughter cysts, indicating viability, have a lower attenuation value than that of mother cysts on CT scans (Fig. 2). On MRI, daughter cysts may appear slightly hypointense or isointense relative to the maternal matrix on the T1-weighted images and hyperintense on the T2-weighted images. When present, floating membranes are seen as low signal intensity linear structures within the cyst on both the T1- and T2-weighted images (2, 3, 8).
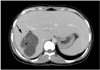
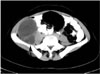
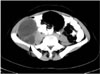
Type III HCs represent a calcified, non-viable degenerated cyst (Fig. 3) (1). US demonstrates cyst calcification as hyperechoic areas with a strong posterior shadow. Cyst calcification can be seen as round, hyperattenuating areas on CT and as hypointense areas on MRI (2, 3).
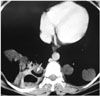
Complications of HC include rupture and superinfection of type I and II cysts (1). Rupture occurs in 50%-90% of cases. Three types of rupture can occur: contained, communicating and direct (1). In contained rupture, the endocyst ruptures and becomes detached from the pericyst. In communicating rupture, the cyst ruptures into an anatomical diversion structure like the biliary or bronchial tree (1). Direct rupture occurs when both the endocyst and the pericyst are ruptured with the cystic contents spilling into the pleural and peritoneal cavities or a hollow viscus (Fig. 4) (1). The cyst may become considerably smaller and less spherical both in communicating and direct ruptures (1). MRI may demonstrate disruption in the low-signal intensity rim of the cyst wall and extrusion of the contents through the defect (3, 8).
LIVER
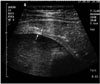
The liver is the most common site of HC. The cysts may cause pain, discomfort, abdominal swelling or a palpable mass or thrill (5, 6). In the early stages of the disease, the appearance of HCs may be uncharacteristic and mimic that of simple cysts. However, the double-line sign can often be seen on sonography in unruptured HCs (Fig. 5) (3, 4). Simple liver cysts do not demonstrate internal structures (2, 3), although multiple echogenic foci due to hydatid sand may be seen within the lesion by repositioning the patient on sonography (Fig. 6) (5). On MRI, a low-signal-intensity rim can be helpful to differentiate a unilocular HC from a simple liver cyst (2). Multiple unilocular cysts are indistinguishable from polycystic disease (2, 5). When echinococcal cysts become enlarged, they can produce pericystic biliary tract dilatation due to the mass effect (Fig. 7) (2, 5, 9). Decreasing intracystic pressure, endocyst degeneration, host response, trauma and medical treatment can cause separation of the endocyst from the pericyst (2, 3). Complete collapse of the endocyst results in a sonographic water-lily sign when the parasite lies in the most dependent part of the cyst or this produces an irregular, solid echo pattern (Fig. 8) (5). The wall of HC, even without calcification, is typically seen as a high-attenuated structure on unenhanced CT (Fig. 1) (3). The calcification may occur in the cyst wall or internally in the cyst, and this is detected on radiography in 20% to 30% of liver HCs (Fig. 3) (2, 3, 5). Following the formation of HC, many potential local complications may develop such as rupture, infection (Fig. 9), perforation to the biliary tree (up to 90% of HCs) (Fig. 10), and involvement of the portal venous system (Fig. 11), diaphragm and thoracic cavity (0.6%-16% of the cases with hepatic HCs) (2, 3).
LUNG
The lung is the second most common location of hematogenous HC spread in adults and it is probably the most common site in children (2, 5). Pulmonary hydatid cysts are often asymptomatic, and they are usually found as incidental findings on routine chest radiography, but occasionally symptoms occur due to the pressure effects on adjacent structures (5). The most prominent radiological finding is a dense, round, well-demarcated opacity that can resemble a neoplasm. Calcification (0.7% of cases) and daughter cysts are rarely seen in lung HD (2, 10). When the growth of the cyst produces erosion in the bronchioles, air between the endocyst and pericyst can produce a "crescent or inverse crescent sign" between the cyst wall and the pericyst (Fig. 12). If air continues to enter the cyst cavity, then the "water lily" sign can be seen (an endocyst membrane floating in the most dependent part of the pericyst cavity) (2, 11). The radiologic appearances of infected cysts are similar to those of a lung abscess: a thick-walled cavity with an air-fluid level and surrounding pneumonia (Fig. 13) (5). When HCs are infected, they can cause a solid appearance and give rise to a diagnostic error such as malignant tumor. Other complications of lung HC include rupture and recurrent acute pulmonary embolism (2).
KIDNEY
Renal HD is rare (3% of case), usually solitary and located in the cortex (2). These patients may present with a flank mass, dysuria, pyuria, hematuria, persistent fever, renal stones, hypertension or renal colic (10). Hydatiduria can occur after rupture of the cyst into the collecting system (5). Any form of HC can be seen in renal HD (Fig. 14) (2, 3, 10). Mural calcification and daughter cysts often coexistent. These findings are helpful in the differential diagnosis of HCs from a simple renal cyst, necrotic renal cell carcinoma, renal abscess and infected cysts, but it sometimes can be difficult to differentiate HC from necrotic renal cell carcinoma since calcifications may be encountered in both lesions (2, 10).
PERITONEAL CAVITY
Peritoneal HC, either primary or secondary, represents an uncommon but significant manifestation of this disease (approximately 13%). It is always secondary to traumatic or surgical rupture of a hepatic, splenic or mesenteric cyst (2, 3, 10). CT is the modality of choice for these patients because it permits imaging of the entire abdomen and pelvis (3). The lesions are generally multiple and any type of HC can arise anywhere in the peritoneal cavity (Fig. 15). Unilocular cysts (type I) should be distinguished from mesenteric cysts or intestinal duplication cysts (2, 6, 10).
SPLEEN
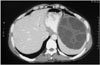
Primary splenic involvement is very rare (less than 2%) (Fig. 16). The symptoms are mainly abdominal pain, splenomegaly and fever. Splenic HCs are usually solitary, and their imaging characteristics are similar to those of hepatic HCs (2, 10). Other splenic cystic lesions such as epidermoid cyst, pseudocyst, splenic abscess, hematoma and cystic neoplasm of the spleen should be considered in the differential diagnosis (10).
PANCREAS
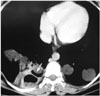
Primary HC of the pancreas is rare, representing 0.2-2% of all human infestation. It is usually single and located in the head of the pancreas (2, 10). The clinical symptoms depend on the size and location of the cyst within the pancreas. The lesion in the head of pancreas frequently presents with jaundice due to obstruction of the common bile duct. However, the body or tail lesions rarely cause symptoms. The differential diagnosis includes abscess or cystic neoplasms of the pancreas (10). The typical appearance and location of HCs within the pancreas is not established due to their relatively rare occurrence (2). In this paper we present the MRI features of primary HC of the pancreas located in the tail (Fig. 17). We also present the CT findings of a partially calcified HC located in the tail of the pancreas (Fig. 18).
ADRENAL GLAND
The adrenal gland is an extremely rare location for HC and it is usually involved as a part of systemic echinococcosis. It is usually asymptomatic and these patients usually present with the symptoms that are caused by space-occupying lesions (12). The imaging features depend on the stage of evolution of the disease (Fig. 19). Unilocular HCs should be differentiated from exophytic renal cysts that originate from the upper pole of the kidney (2).
OVARY
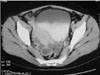
Ovarian involvement is also very rare and generally secondary to peritoneal spread of daughter cysts due to rupture of a liver HC. Ovarian HCs are usually asymptomatic and they can be discovered incidentally or they may cause irritation or compression symptoms. The ovarian lesion may be unilocular (Fig. 20) or contain daughter cysts that can give rise to a multiloculated appearance, and ovarian lesion should be considered in the differential diagnosis of cystic pelvic masses such as cystadenoma or cystadenocarcinoma (2).
RETROPERITONEUM
Isolated retroperitoneal HCs are also uncommon and they are usually secondary to the involvement of other organs or to previous surgery. Any type of HC can be seen in the retroperitoneum (2, 13). In this paper we present the CT findings of a case of retroperitoneal type II HC that originated from the right psoas muscle (Fig. 21). There was no evidence of any other organ involvement in this case.
MEDIASTINUM
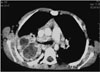
Mediastinal HCs are also rare and they can be solitary or multiple lesions. The symptoms and complications of cyst depend on the size, location and involvement of adjacent structures. The imaging appearance can vary from type I to type III (2) (Fig. 23). The HCs in the mediastinum should be differentiated from cysts of a bronchogenic, pleuropericardial, thymic or enteric origin, and from intramural esophageal cysts such as lymphangioma and anterior meningocele (3).
CONCLUSION
The occurrence of E. granulosus in some locations of the body is very rare. These anatomic locations may cause difficulties in making the differential diagnosis as E. granulosus is usually not suspected in some locations of the body. Imaging modalities such as US, CT and MRI are helpful in diagnosing this disease. Radiologists, surgeons and physicians should always consider HD in differential diagnosis of a cystic lesion, and especially for the cystic leasions encountered in patients who live in or have come from endemic regions and if any of the previously described imaging features (e.g., calcification, daughter cysts and/or intracystic membranes) are seen. Familiarity with the various imaging appearances of HD may prevent diagnostic delay, and so decrease the risk of life-threatening complications.












 XML Download
XML Download