

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Takayasu arteritis is a systemic vasculitis that mainly involves the large arteries, including the aorta, the pulmonary artery and their branches. The disease is divided into two phases: the early systemic phase and the late occlusive phase (1, 2). In its occlusive phase, the diagnosis is evident by the characteristic ischemic symptoms and the typical angiography. The typical angiographic findings include a diffuse luminal narrowing or occlusion of the thoracic or the abdominal aorta and involvement of the major branches (3, 4). However, the diagnosis is difficult in its systemic phase, with patients displaying generalized weakness and a fever of an unknown origin. CT may reveal the mural changes even in the early systemic phase, without any noticeable arterial occlusive changes (5, 6). Those are the mural thickening and enhancement of the aorta, the pulmonary artery and their branches. The activity of the disease may be controlled with steroid and immunosuppressive drugs (5, 7). During the follow-up period, in case of active disease, the CT findings may show changes after appropriate treatment. Follow-up CT evaluation may be useful for evaluating the response to treatment, and to demonstrate the mural or luminal changes that can be traced in time (8).
We performed this retrospective study to evaluate the mural changes of the CT findings in patients who initially had active Takayasu arteritis and they later underwent follow-up CT examination more than one time.
MATERIALS AND METHODS
A total of 220 patients with Takayasu arteritis underwent CT examinations in our hospital during the 12 years, from January 1994 to December 2005. To satisfy the inclusion criteria, the patients had to have active Takayasu arteritis and to have had the follow-up CT examination done. The criteria for the active disease at the time of the initial CT included systemic features, an elevated erythrocyte sedimentation rate (ESR, normal range in females: 0 20 mm/hr, in males: 0 9 mm/hr) and abnormal mural changes according to the initial CT evaluation.
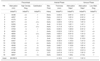
Eighteen patients were included in this retrospective study to evaluate the interval changes of the CT findings in Takayasu arteritis. Four of them were males and 14 were females. Their ages ranged from 11 to 53 years, with the mean age of 31.2 years at the time of the initial CT examination. From two to four CT examinations were performed in each patient. The total number of the CT examinations was 44. The follow-up periods ranged from 10 months to 10 years four months. The mean follow-up period was 55.6 months. The clinical findings of the 18 patients are summarized in Table 1, including the number of the CT examinations, the modified Ueda type of extent of disease, the levels of ESR and C-reactive protein, along with the medical and surgical or interventional treatments. The ESR was elevated in all except two patients (Cases 1 and 8), who showed an elevated ESR on a repeated examination performed within one month. The course of disease was modified Ueda type I in four patients, type II in two patients, type III in nine patients and type IV in three patients. All the patients, except one patient with active pulmonary tuberculosis, were treated with prednisolone alone, or with methotrexate or cyclophosphamide. By the follow-up evaluation, the disease was defined as inactive if the ESR was normal at least for six months without steroid medication. Otherwise, the disease was defined as active. According to the above criteria, the disease was active in all 18 patients at the time of the initial CT evaluation. The disease was considered as inactive in five patients and active in 13 patients at the time of the last follow-up CT.
CT Techniques
Because of the long period for collecting the cases, more than 10 years, various CT scanners were used for the patients scanning; these scanners varied from a single slice spiral CT to a 16-channel multidetector CT (MDCT) scanner including single slice spiral CT (Somatom Plus-S, Somatom Plus-4, Siemens, Erlangen, Germany), the 4-channel MDCT (MX8000, Marconi Medical Systems, Cleveland, OH), the 8-channel MDCT (LightSpeed Ultra, GE Medical Systems, Milwaukee, WI) and the 16-channel MDCT (Sensation 16, Siemens, Erlangen, Germany).
An 18-, or 20-gauge needle was placed into the antecubital vein, and 150 ml of nonionic contrast material, iopromide (Ultravist 370; Schering, Berlin, Germany) was injected at a rate of 2.5 3.0 ml/sec with using a power injector (Envision CT; Medrad, Indianola, PA). We used the bolus-tracking method at the ascending aorta level and set 100 HU as the triggering threshold for the arterial phase. The venous phase scan was taken at 5 to 10 minutes after initiating the injection of the contrast material.
The scanning parameters varied according to the type of the scanner, but the following basic concept for scanning of the aorta was followed: the slice thickness was kept as thin as possible for the scanning phase of the precontrast phase, the arterial phase and the venous phase. For the arterial phase, the slice thickness was 3 mm on the single spiral CT and the 4-channel MDCT with 2 mm reconstruction intervals, and it was 1.5 mm on the 8-channel and the 16-channel MDCT with 1 mm reconstruction intervals. For the precontrast and the delayed venous phase scans, the slice thickness was 5 mm on the single spiral CT and MDCT. The pitch value was 2 for the single spiral CT and 1 to 1.5 for MDCT. MDCT could cover the whole aorta during the time of a single breath-hold, and each scan was done with a single breath-hold. In case of the single slice spiral CT, the whole aorta for the arterial phase was covered with two breath-hold scans, one for the thoracic aorta and the other for the abdominal aorta.
The Data Analysis
The high density of the aortic wall and the mural calcification on the precontrast CT scan and the low-attenuated ring on the arterial and the venous phase CT scan were examined by two collaborating radiologists. The mural findings of the follow-up CT were compared with those of the initial CT. In cases of multiple follow-up evaluations, the findings of the latest CT were compared. The two radiologists measured the mural thickness on the transverse image of the arterial phase and the CT attenuation of the aortic wall in the precontrast, arterial and venous phases. The mean CT attenuation value in Hounsfield units was calculated based on three or more measurements with a region of interest of 2-7 mm2. The measurement was performed at the location with a maximum mural thickness, including the ascending aorta, the arch, the left common carotid and abdominal aorta.
The arterial and delayed enhancements of the aortic wall were compared with the attenuation of the back muscle of the same image, and this was expressed as a ratio. The ratio of the attenuation of the enhanced aortic wall over the attenuation of the back muscle in the initial CT was compared with that of the follow-up CT. The luminal findings, in addition to the mural changes, were also considered on the initial and follow-up CT examinations.
For the statistical tests between the two groups, Mann-Whitney U test was used for continuous variables, and the Fisher exact test was used for categorical variables. The Wilcoxon signed rank test was applied for statistically testing the follow-up evaluation. A two-tailed p value of 0.05 or less was considered to indicate statistical significance, and SPSS 10.0 statistical computer software (SPSS, Chicago, IL) was used.
RESULTS
The Initial CT Findings
The mural changes found on the initial and follow-up CT evaluations of the 18 patients are summarized in Table 2.
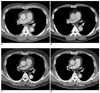
On the precontrast CT, the high density of the aortic wall was noted in 15 patients (83%). Curvilinear or dot-like calcifications were found in six patients (33%). On the arterial phase of CT, the aortic wall was thickened with the mean thickness of 4.1 mm. The wall was slightly enhanced in various portions of the aorta and its branches, and the mean ratio of attenuation of the wall over that of the back muscle was 1.4. A circumferential low-attenuation ring was demonstrated for the patients with substantial arterial enhancement. In the venous phase, the mural enhancement was more pronounced in all the patients with an attenuation ratio from 1.2 to 2.6 (the mean value: 1.9). The low-attenuation ring was well demonstrated between the contrast-filled lumen and the enhanced outer wall in 15 patients (83%) in the venous phase (Fig. 1).
No significant stenosis was shown, even for the four patients with significant mural changes. Variable degrees of the luminal changes, including stenosis and dilatation, were noted in the aorta and its branches in 14 patients.
The Follow-up CT findings (Tables 2, 3 and 4)
On the follow-up CT evaluation, with a mean follow-up period of 55.6 months, the precontrast image showed the high density ring in two more patients (Table 2). The mean attenuation (HU) of the aortic wall on the precontrast phase increased significantly from 48.9 to 56.5 (p = 0.04) (Table 3). The mural calcifications noted in 10 patients were more extensive. The mean mural thickness measured on the arterial phase was 2.4 mm, and it was significantly decreased from 4.1 mm as measured by the initial CT evaluation (p = 0.001). The mean CT attenuation ratio of the wall (aortic wall/muscle) in the venous phase decreased significantly from 1.9 to 1.3 (p = 0.001). The low-attenuation ring in the venous phase was identified in seven patients (39%) with active persistent disease.
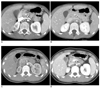
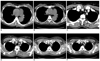
The mural thickness decreased, and the mural enhancement also decreased significantly in both the group of patients with inactive disease and in the group of patients with active persistent disease (Figs. 2, 3). In the group of the inactive disease patients (n = 5), the low-attenuation ring, initially shown in four patients (80%), disappeared in all the patients by the last follow-up CT (Fig. 2). However, each of the individual CT findings had no statistically significant correlation with the ESR-based disease activity on comparison between the both groups.
Luminal stenosis was improved along with the mural changes by the follow-up CT after medical treatment in two patients (Cases 7 and 16). In one patient (Case 1), the lumen of the abdominal aorta and the proximal left renal artery had recovered, while focal stenosis developed at the middle of the left renal artery. The luminal changes are summarized in Table 4.
DISCUSSION
Various imaging modalities may reveal the mural changes in patients with Takayasu arteritis during the early phase of the disease with or without such luminal changes, as dilatation and stenosis (6, 8-10). CT may reveal mural thickening with the arterial and venous enhancement (5, 6, 8, 9). Sonography shows a homogenous concentric mural thickening of the aorta and its branches, such as the carotid or subclavian arteries (9, 11). The MR imaging reveals the mural thickening of the aorta, the pulmonary artery and its branches, and especially on the gadolinium enhanced T1 weighted images. The mural thickening and the enhancement, as evaluated by each modality, may decrease after appropriate treatment (9-13).
In this retrospective study, we evaluated the mural changes on the follow-up CT examination for the patients with active disease at the time of the initial CT examination. There have been a few reports on the detailed analysis of the mural changes on the follow-up CT evaluation in a group of patients. Paul et al. reported on their results of electron beam CT follow-up, in which they noted a decrease of the mural thickening and an increase of the mural calcifications. The outer wall enhancement, initially noted in 81% cases, was found in 37% case on the last CT scans (8). For our results, the mural thickness decreased significantly from 4.1 mm to 2.4 mm. Other mural changes seen on the follow-up CT evaluation included increased attenuation of the aortic wall and more extensive mural calcifications on the precontrast CT. The mural enhancement in the venous phase was decreased significantly on the follow-up CT evaluation.
It is very difficult to estimate the activity of this disease with using a single parameter of the clinical or imaging diagnosis. There are 4 criteria for the disease activity: systemic features, an elevated ESR, features of vascular ischemia and the typical angiographic features (7). Systemic features such as neck or shoulder pain may fail to represent the real activity of the disease.
One of the criteria is the typical angiographic features. However, the conventional angiography may show only the luminal changes. The angiography may be normal even with an extensive wall thickening if the mural changes did not cause luminal changes, such as narrowing, irregularities or aneurysm (6, 9). So, any cross-sectional imaging modality, including sonography, CT and MR, may be added to make the criteria of activity complete in respect of the angiographic feature. The disease should be regarded as active if there is any new focus or an aggravation of the mural changes according to a cross-sectional imaging modality. On the contrary, the mural changes may resolve completely with appropriate treatment, resulting in an inactivated form of disease. Choe et al. reported that the contrast-enhanced MR imaging showed more enhancement of the thickened aortic wall as compared with the myocardium, suggesting active disease. For determining the progress of the disease activity, they reported an agreement rate for contrast-enhanced MR imaging as 88.5% with the clinical findings: 92.3% with the ESR and 84.6% with the C-reactive protein (13).
In this study, the disease was defined as inactive by the follow-up evaluation if the ESR was normal at least for six months even without steroid medication. After appropriate treatment, the mural thickness decreased significantly in all five cases with inactive disease, as was established by the follow-up CT evaluation. The wall enhancement in the delayed venous phase also decreased significantly in those patients.
For the microscopic findings of Takayasu arteritis, the inflammatory reactions affect mainly the adventitia and the media. The intima shows no inflammatory process. The intimal thickening is a secondary reactive phenomenon. In the acute phase, the media shows vascularization, and the capillaries originating at the transition zone of the adventitia proliferate to the entire medial layer. Following this neovascularization, inflammatory tissue invades the media with infiltration of lymphocytes, plasma cells and giant cells (14). The active inflammation of the outer wall contributes mainly to the thickening of the aortic wall in the early phase of Takayasu arteritis. The mural enhancement in the arterial or venous phase is most likely associated with the neovascularization and the productive inflammation of the media and the adventitia. The intima is thickened with an increase of the basophilic ground substance during the acute phase (14). It can be seen as a radiolucent ring with a good contrast between the enhanced outer wall and the contrast filled arterial lumen. An improvement of the inflammatory process of the aortic wall may be manifested as a decrease of the thickness, a decrease of the mural enhancement and disappearance of the inner low-attenuation ring on the follow-up CT evaluation.
CT may reflect the mural changes on the follow-up evaluation of active Takayasu arteritis. However, there was no statistical significance in the correlation between the CT findings and activity of the disease on the basis of the ESR in this study. Though the ESR is a sensitive parameter of active inflammation, it is nonspecific and has certain limitations in representing the activity of this disease. The ESR has been reported to be persistently elevated during clinical remission in 56% of the cases (7).
The CT protocol in this study was variable because different CT scanners were used for the patients who were selected retrospectively over a long period. On the CT angiography for patients with Takayasu arteritis, the carotid bifurcation should be included into the examination because involvement of the common carotid artery is common in Takayasu arteritis. This coverage gives us useful information about the carotid circulation with the collateral pathways. The thinner the slice thickness is, the easier it is to detect stenosis of the aortic branches such as the renal artery. In addition to the arterial phase data, the venous phase imaging also reveals important mural changes, including the delayed enhancement and the inner low-attenuation ring. However, the thin section acquisition and the additional venous phase imaging may be associated with exposure of patients to a considerable dose of radiation. Decreasing the tube current and increasing the slice thickness up to 5 mm in the venous phase may diminish the radiation dose (15, 16).
There are certain drawbacks or limitations of this study. It was a retrospective study of CT follow-up in patients with Takayasu arteritis with the different intervals between the initial and the CT follow-up examinations being from 10 months to 10 years. There could be bias in selection of the patients with active Takayasu arteritis since the clinical criteria of activity were not perfect. The number of cases was not adequate to provide a sufficient statistical analysis with many CT findings. The CT imaging protocols and the imaging systems were not identical, which was due to the evolution of the CT technology during the study period. The regimen and the dosage of the medical treatment were different because the patients included into the study were treated by different clinicians.
In summary, the mural changes on the follow-up CT evaluation of patients with active Takayasu arteritis include a decrease of the mural thickness, a decrease of the mural enhancement and disappearance of the low-attenuation ring in the venous phase, and an increase of the mural attenuation and calcifications in the precontrast phase. Further investigations are necessary to establish the correlation between these mural changes noted over a period of time with the luminal changes and the long-term prognosis of patients with active Takayasu arteritis.



 XML Download
XML Download