

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Screening for lung cancer using chest CT is becoming more prevalent, and small peripheral lung cancers are being detected more frequently. According to the results of early data from the Early Lung Cancer Action Project, 19% of positive findings on baseline screening CT were due to nodules manifesting as ground-glass opacity (GGO) (1). Histologically, most nodular GGOs are well differentiated bronchioloalveolar-type adenocarcinomas, bronchioloalveolar carcinoma (BAC), or atypical adenomatous hyperplasia (AAH) (1, 2).
The nodular GGO is a wispy, diagnostically frustrating pulmonary infiltrate, which is being detected with increasing frequency as the resolution of CT improves. Physicians are therefore increasingly asked to diagnose, manage and treat nodular GGO discovered by CT scanning. Moreover, it is also known that the frequency of malignancy in nodular GGO, including the solid portion, was much higher than in solid nodules (1, 2). However, there is suspicion that nodular GGO may represent over diagnosis of lung cancer because it progresses so slowly it may be inconsequential. Because of the short history of this new entity, its natural history is unknown; thus a standard diagnostic scheme and treatment strategies have not been fully established. However, if we knew the factors that influence the progression of the lesion and the malignant potential, there would be no need to hesitate on decisions regarding surgical resection or follow-up without intervention. The size, internal solid portion and the morphology of the lesion may be considered as the factors important for such decisions. Among the possible factors, we examined the significance of the size and focal solid potions of the nodular GGOs in this study. Therefore, the purpose of this study was to evaluate the inter-group difference in the pattern of growth and the pathological results of nodular GGOs after classification of the lesions according to the size and focal solid portion.
MATERIALS AND METHODS
Patients
From September 2002 to July 2005, nodular GGOs smaller than 3 cm were found on chest CT in 93 individuals; follow-up thin-section CT (1-2.5 mm) were performed in 64 individuals. Six lesions in six individuals were confirmed as solid nodules on thin-section CT. Three lesions in three individuals disappeared at the one-month follow-up with thin-section CT. The remaining 96 nodular GGOs in 55 individuals (M:F = 27:28; age range 44-80; median age 58; mean age 59) were included in this study. The lesions were followed by CT for at least one month from the initial chest CT (1-49 months, mean 7 months). Forty nodular GGOs in 30 individuals were pathologically confirmed to be: adenocarcinoma (n = 15), BAC (n = 11), AAH (n = 8), focal interstitial fibrosis (n = 5) and aspergillosis (n = 1) by lobectomy (n = 30), wedge resection (n = 9) and cutting needle biopsy (n = 1). Fifty-six nodular GGOs in 25 individuals are currently being followed by CT. Because of the retrospective nature of this study, the decision for surgical biopsy was not based on documented protocol. Management decisions were made on a case by case basis with published data (1) and through conference with physicians and surgeons.
Patients with peripheral blood eosinophilia or the possibility of hemorrhagic metastasis were excluded. Thirty-eight individuals were non-smokers, 15 were current smokers and two were ex-smokers. The lesions were incidentally found in 53 individuals by regular screening or as part of the evaluation of other diseases, one was found by imaging work-up for hemoptysis, and another by CT imaging for persistent whitish sputum. Eight individuals had a history of a previous malignancy in a variety of organs: stomach cancer (n = 2), bladder cancer (n = 2), breast cancer (n = 1), chondrosarcoma (n = 1), osteosarcoma (n = 1), and malignant fibrous histiocytoma (n = 1). Three individuals had a concurrent adenocarcinoma with a solid mass in other lobes of the lung.
CT Imaging
In all individuals, a thin-section CT was performed at least one time during the follow-up. In 24 individuals, thin-section CT was performed with a LightSpeed-Ultra scanner (GE Medical Systems, Milwaukee, WI) with 120 kVp, 400 mAs, a pitch of 0.875, and collimation of 1.25 mm. Images were reconstructed with 1.25 mm thickness. In 18 individuals, thin-section CT was performed with a Sensation-16 scanner (Siemens Medical Solutions, Erlangen, Germany) with 140 kVp, 250 effective mAs, pitch of 1, and collimation of 0.75 mm. Images were reconstructed with 1 mm thickness. In four individuals, thin-section CT was performed with a MX 8000 scanner (Phillips Medical Systems, Netherlands) with 120 kVp, 150 mAs, pitch of 1.25, and collimation of 2.5 mm. Images were reconstructed with 2.5 mm thickness. In five individuals, thin-section CT was performed with a Somatom plus-4 (Siemens Medical Solutions) with 120 kVp, 300 mAs, pitch of 1, and collimation of 1-2 mm. Images were reconstructed with 1-2 mm thickness. In the remaining four individuals, the thin-section CT was performed at outside institutions with a variety of scanners with 120-140 kVp, 200-300 mAs, pitch of 1-1.5, collimation of 0.75-2.5 mm, and reconstruction thickness 0.75-2.5 mm. In all individuals, scanning was performed at end inspiration following hyperventilation.
Initial or follow-up chest CT was performed using a variety of scanners including: Sensation-16, LightSpeed-Ultra, MX-8000, Somatom plus 4, or HiSpeed Advantage (GE Medical Systems). Chest CT was performed with 120 kVp, 200-300 mA, pitch of 0.875-1.5, and collimation of 0.75-8 mm. Images were reconstructed using high-frequency algorithms with 1-8 mm thickness.
Image Reading and Data Analysis
The CT images were read by three board-certified radiologists in consensus, each of whom had more than eight years of experience in chest image interpretation. The consensus results were documented. The number of nodular GGOs at the initial CT and the presence of mediastinal lymph node enlargement were initially evaluated.
We classified each lesion as to its type-pure nodular GGO (PNGGO) or mixed nodular GGO (MNGGO)-on the basis of the appearance on the thin-section CT scans. A lesion was classified as MNGGO if it contained patches that completely obscured the lung parenchyma. A lesion was classified as PNGGO if none of the lung parenchyma within it was totally obscured. In making the distinction between a PNGGO and a MNGGO, we did not regard blood vessels as solid components despite their solid appearance.
The diameter of a nodule, as a measure of its size, was defined as the average of its length and width measured with electronic calipers on the image that showed the largest cross-sectional area of the nodule. The diameter was measured on the initial chest CT and on the final chest CT.
Subsequently, we categorized nodular GGOs into four groups on the basis of the size on initial CT and type on the thin-section CT: PNGGO ≤ 10 mm, PNGGO > 10 mm, MNGGO ≤ 10 mm, and MNGGO > 10 mm. In each group, we evaluated the change in size during the follow-up period, and the pathological result. The rate of malignancy and rate of adenocarcinoma were calculated on a lesion by lesion basis.
We graded the area of the solid portion in MNGGOs on the thin-section CT scans with a four-point scale. Grade 1 was defined as a solid portion ≤ 25%, grade 2 as a solid portion ≤ 50%, grade 3 as a solid portion ≤ 75% and grade 4 as a solid portion > 75%. The change of size during the follow-up period and the pathological results according to the grade of solid portion was assessed. The rate of malignancy and the rate of adenocarcinoma according to the grade of solid portion were also evaluated.
Go to : 
RESULTS
Forty-three individuals had a single lesion, five had two lesions, two had three lesions, two had four lesions, one had eight lesions, one had nine lesions and one had 12 lesions. In 12 individuals who had multiple lesions, nine had only PNGGO and three had both types of GGOs. None of the individuals had lymph node enlargement in the mediastinum. The initial size of the 96 nodular GGOs was 2-30 mm (mean, 9.7 mm).
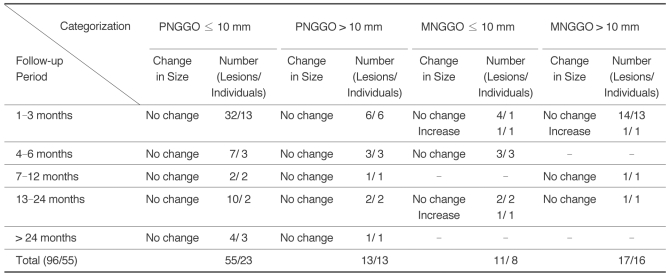
The results of categorization and change of size are presented in Table 1. Fifty-five lesions in 23 individuals were PNGGO ≤ 10 mm and 13 lesions in 13 individuals were PNGGO > 10 mm. Eleven lesions in eight individuals were MNGGO ≤ 10 mm and 17 lesions in 16 individuals were MNGGO > 10 mm. For the PNGGOs, a change of size was not noted in any lesion during follow-up (Fig. 1). Two lesions in the MNGGOs ≤ 10 mm and one lesion in the MNGGOs > 10 mm grew in size during the follow-up period.
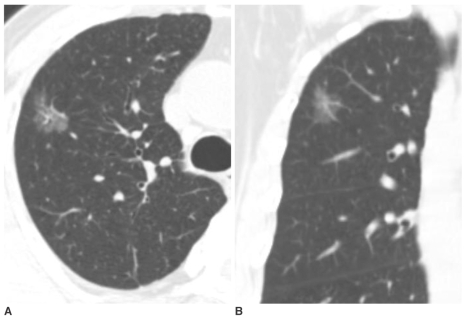
 | Fig. 1Pure nodular ground-glass opacity in the right upper lobe confirmed as atypical adenomatous hyperplasia in a 62-year-old woman.
A. Initial CT shows 8 mm pure nodular ground-glass opacity in the right upper lobe.
B. Thin-section CT after 10 months shows persistent pure nodular ground-glass opacity with the same size. The lesion was pathologically confirmed by right upper lobectomy. She had a history of curative resection of adenocarcinoma in the left upper lobe one year before.
|
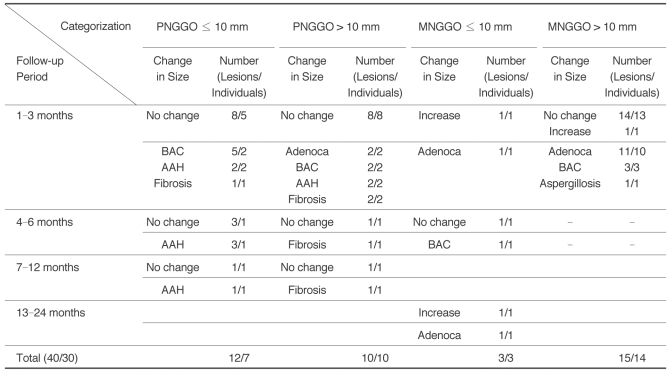
Twelve lesions from the PNGGOs ≤ 10 mm, ten lesions from the PNGGO > 10 mm, three lesions from the MNGGO ≤ 10 mm and 15 lesions from the MNGGO > 10 mm were resected. The histological results and change of size in each group are presented in Table 2. The resected PNGGOs ≤ 10 mm were AAH (n = 6) (Fig. 1), BAC (n = 5), and focal interstitial fibrosis (n = 1). The resected PNGGOs > 10 mm were focal AAH (n = 2) (Fig. 2), BAC (n = 2), adenocarcinoma (Fig. 3) (n = 2) and interstitial fibrosis (n = 4) (Fig. 4). The resected MNGGOs ≤ 10 mm were adenocarcinoma (n = 2) and BAC (n = 1). The resected MNGGOs > 10 mm were adenocarcinoma (n = 11) (Fig. 5), BAC (n = 3) and aspergillosis (n = 1) (Fig. 6). Three lesions that had grown during the follow-up were histologically confirmed as adenocarcinoma with mixed acinar and bronchioloalveolar patterns. Among 15 adenocarcinomas, 13 lesions were histologically confirmed as well-differentiated or moderately-differentiated adenocarcinoma with mixed acinar and bronchioloalveolar types and two were as well-differentiated adenocarcinoma with bronchioloalveolar type.
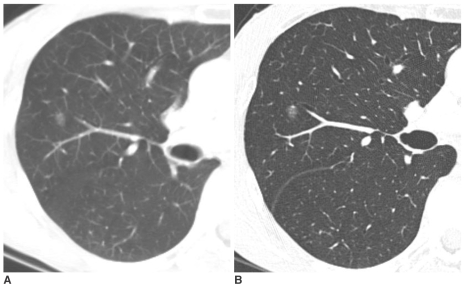
 | Fig. 2Pure nodular ground-glass opacity in the right upper lobe confirmed as atypical adenomatous hyperplasia in a 58-year-old man.
A. Initial thin-section CT shows a 15 mm pure nodular ground-glass opacity in the right upper lobe.
B. On thin-section CT after 2 months, an interval change was not noted. An additional two pure nodular ground-glass opacities were found in the right upper lobe and one in the right middle lobe. All lesions were pathologically confirmed as atypical adenomatous hyperplasia by multifocal wedge resection.
|
 | Fig. 3Pure nodular ground-glass opacity in the right upper lobe confirmed as adenocarcinoma in a 67-year-old man.
A, B. Axial and coronal-reformatted images of thin-section CT shows 25 mm pure nodular ground-glass opacity in the right upper lobe. The lesion was pathologically confirmed by right upper lobectomy.
|
 | Fig. 4Pure nodular ground-glass opacity in the right upper lobe confirmed as focal interstitial fibrosis in a 61-year-old man.
A. Thin-section CT shows 30 mm pure nodular ground-glass opacity in the right upper lobe.
B. On follow-up CT scan after seven months, an interval change was not noted. The lesion was pathologically confirmed by right upper lobectomy. On pathologic slides, focal interstitial fibrosis with exuberant type II pneumocyte proliferation and alveolar macrophage collection were found. The cause of the focalinterstitial fibrosis was not confirmed.
|
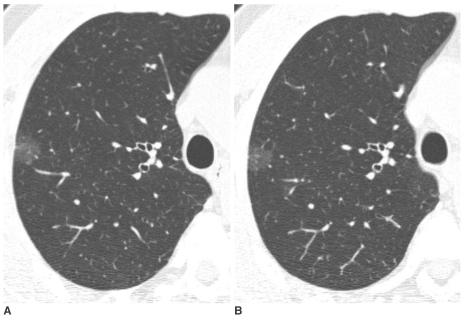
 | Fig. 5Mixed nodular ground-glass opacity in the right lower lobe confirmed as adenocarcinoma in a 61-year-old man.
A, B. Axial and coronal-reformatted images of thin-section CT shows 21 mm mixed nodular ground-glass opacity in right upper lobe. An elongated shaped solid portion was noted in the lesion (arrows). The lesion was pathologically confirmed by right lower lobectomy.
|
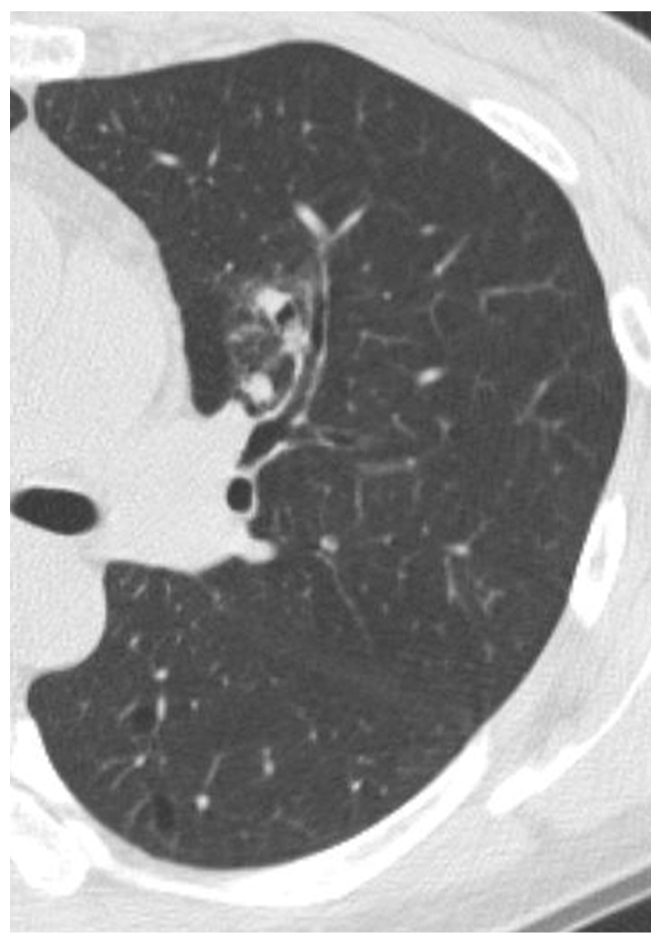 | Fig. 6Mixed nodular ground-glass opacity in the left upper lobe confirmed as aspergillosis in a 52-year-old woman. Thin-section CT shows 23 mm mixed nodular ground-glass opacity in the left upper lobe. Multifocal solid portions were seen in the lesion. The lesion was pathologically confirmed by CT-guided cutting needle biopsy. She also had fungal sinusitis in the right maxillary sinus.
|
Table 2
The Pathology of Nodular Ground-Glass Opacities and Change of Size during the Follow-up Period
Note.-GGO = ground-glass opacity, PNGGO = pure nodular ground-glass opacity, MNGGO = mixed nodular ground-glass opacity, BAC = bronchioloalveolar carcinoma, AAH = atypical adenomatous hyperplasia, Adenoca = adenocarcinoma, Fibrosis = focal interstitial fibrosis
The sum of patient number is not matched with total number because of the patients with multiple lesions.
![]()
In the resected lesions, the rate of malignancy on a lesion basis was 42% (PNGGOs ≤ 10 mm), 40% (PNGGOs > 10 mm), 100% (MNGGOs ≤ 10 mm) and 93% (MNGGOs > 10 mm). The rate of adenocarcinoma was 0% (PNGGOs ≤ 10 mm), 20% (PNGGOs > 10 mm), 67% (MNGGOs ≤ 10 mm) and 73% (MNGGOs > 10 mm).
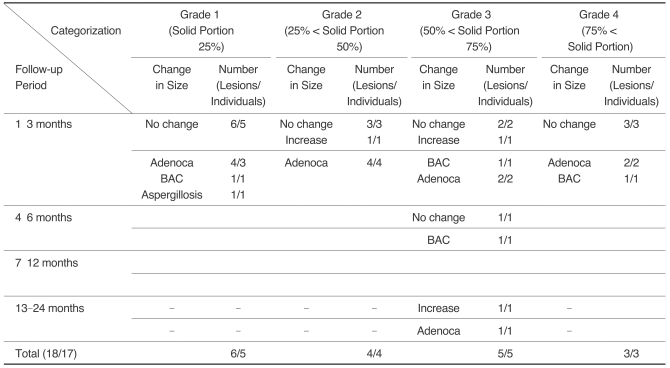
The pathology and change in size during the follow-up period according to the grade of the solid portion in the MNGGOs are presented in Table 3. One lesion that had grown during the follow-up was grade 2, another was grade 3, and a third was grade 4. According to the grade of the solid portion of the MNGGOs, the rate of malignancy on a lesion by lesion basis was 83% (grade 1) and 100% (grades 2-4). The rate of adenocarcinoma was 67% (grade 1), 100% (grade 2), 60% (grade 3) and 67% (grade 4).
Go to :
DISCUSSION
The results of this study can be summarized as the following: a) None of the PNGGOs showed considerable change in size during the follow-up period; b) Most of the PNGGOs were histologically AAH, BAC, or focal interstitial fibrosis; c) We did not find adenocarcinoma among PNGGOs ≤ 10 mm but, there were several adenocarcinomas among PNGGOs > 10 mm; d) Several MNGGOs grew during the follow-up period and they were histologically described as adenocarcinoma; e) In MNGGOs, the possibility of malignancy and the possibility of adenocarcinoma were high, regardless of the grade of the solid portion.
In this study, we introduced the term "nodular GGOs". The term "ground-glass" was introduced to describe not only focal abnormalities but diffuse abnormalities as well. Therefore, the adjective "nodular" was added. "Nodular GGOs" is more appropriate than "focal GGOs" or "localized GGOs" because the latter also represents nonspecific irregular infiltration or mosaic attenuation of the lung.
Pure Nodular Grand-Glass Opacities
The Change in Follow-up
In the current study, PNGGOs remained stable over a considerable time. None of PNGGO showed a change in size during the follow-up period regardless of size. A long doubling time for PNGGOs is already known. Hasegawa et al. (3) reported a mean volume doubling time for PNGGO tumors to be 813 days, which was significantly longer than for MNGGO tumors with a solid central component (457 days) or in entirely solid nodules (149 days). Aoki et al. (4) reported that all adenocarcinomas with Noguchi types A (localized BAC) or B (localized BAC with foci of structural collapse of alveoli) tumors with localized GGO (5) on high-resolution CT had a tumor doubling time of more than one year. Kodama et al. (6) reported that, among 19 PNGGOs over a two-year follow-up, the size increased by more than 5 mm in five patients, increased up to 5 mm in six patients and showed no change in eight patients. The resected lesions were histologically BAC, adenocarcinoma, AAH, focal fibrosis and lymphoproliferative disease. Kodama et al. did not describe the CT parameters and the method of measurement in their article. Many of the lesions were inflammatory lesions such as lymphoproliferative disease. The discrepancy between our results and those of Kodama et al. might be caused by the difference in the follow-up period, the method of measurement and CT parameters and the difference in the disease entities studied. Kakinuma et al. (7) reported that eight PNGGOs over six-months changed during follow-up; five increased in size, two decreased and one was stable in size with increasing density. The discrepancy between our results and those of Kakinuma et al. can be explained by the difference in patient selection. We included all of the PNGGOs incidentally detected by CT. By contrast, Kakinuma et al. only enrolled the PNGGOs that were histologically confirmed as lung cancer and were larger than 5 mm in diameter at the time of the first thin-section CT. Moreover, in most of the PNGGOs described by Kakinuma et al., the focal solid portion appeared during the follow-up, and growth occurred after the appearance of a focal solid portion. Therefore the growth occurred when the nodule was a MNGGO not a PNGGO (7).
The Potential of Malignancy
Most of the PNGGOs in this study were histologically AAH, BAC or focal interstitial fibrosis. Among PNGGOs smaller than 10 mm, there were no cases of adenocarcinoma. Two cases of PNGGOs larger than 10 mm were adenocarcinoma. Theoretically, PNGGOs on high resolution CT (HRCT) should not possess a nonaerated component suggesting adenocarcinoma in their pathologic specimens, since nonaerated components usually appear as focal solid portions on HRCT. This discrepancy may have developed from partial volume averaging due to relatively thick CT slices. One of two adenocarcinomas appeared as a PNGGO on CT scanned with 2.5 mm slice thickness. By contrast, other PNGGOs were scanned with 1-1.25 mm slice thickness. The sizes of the nonaerated component of the resected adenocarcinomas were smaller than 3 mm. Nakajima et al. (8) reported that 10% of PNGGO lesions were adenocarcinoma with stromal invasion. They obtained HRCT images with 2 mm slice thickness. Therefore, the detection of small nonaerated components, which enable AAH or BAC to be distinguished from adenocarcinoma, may be difficult with 2-2.5 mm slice CT. To discriminate between adenocarcinoma, BAC and AAH, a much higher resolution CT examination is needed.
Usually, a focal GGO due to acute inflammation or bleeding disappears during a three month follow-up period. However, PNGGOs due to focal interstitial fibrosis remained stable over a several months in our study. These lesions were histologically confirmed as focal interstitial fibrosis with fibroblast and type II pneumocyte proliferation and collection of alveolar macrophages. Previous investigators have suggested that a polygonal or flat shape of the lesions represent advanced scar tissue as a result of an inflammatory process from a variety of causes and that the possibility of malignancy or AAH is substantially low (9).
Treatment Strategy of Pure Nodular Grand-Glass Opacities
In this study the PNGGO smaller than 10 mm remained stable for a considerable period of time. This data suggest that most small PNGGOs might not progress to clinical disease and may be included in the category of over diagnosis bias. However, we still cannot recommend follow-up thin-section CT without immediate diagnostic intervention because of the discrepancy with previous reports (6, 7). By contrast, when the PNGGO is larger than 10 mm or shows an increase in size or density, wedge resection of the lesion should be recommended for the purpose of a diagnostic intervention as choice of management. Although, transthoracic CT-guided biopsy has frequently offered an alternative to open surgical biopsy for preoperative diagnosis, there are drawbacks to transthoracic biopsy. For the differentiation of AAH, BAC and adenocarcinoma, an adequate tissue sample including the entire area of the lesion should be obtained. In addition, BAC cannot be diagnosed based on a small biopsy sample because the definition of BAC requires that there be no evidence of invasive features within the entire lesion (10). Moreover, three different kinds of histological components could be mixed in a lesion with variable proportions and focal adenocarcinoma can be missed with transthoracic biopsy.
Mixed Nodular Grand-Glass Opacities
The Change in Follow-up and the Potential of Malignancy
The MNGGO has potential for growth. In the current study, all lesions that grew in size during the follow-up were adenocarcinoma. These results suggest that MNGGO may be a radiological manifestation of advanced cancer with a short doubling time compared to PNGGO, which is supported by results of a previous study (3). Our study also showed that, regardless of the initial size of the lesion, the rate of malignancy and the rate of adenocarcinoma were high with the MNGGOs. Our results are consistent with the report by Henschke et al. (1). They reported that, the frequency of malignancy in MNGGO was much higher than in solid nodules, and that the distribution by malignancy type was strikingly different in the MNGGOs as compared with solid nodules. The malignancies in MNGGOs were typically BACs or adenocarcinomas with bronchioloalveolar features, whereas for the solid nodules the malignancies were typically other subtypes of adenocarcinoma.
According to the 1999 WHO classification, BAC is defined as a noninvasive tumor in adenocarcinoma (10). AAH has been suggested to be a possible precursor to BAC, and many studies have been conducted to characterize AAH (11-16). Both AAH and BAC without fibroblast proliferation display a replacement growth pattern. Theoretically, these lesions should therefore exhibit PNGGOs on HRCT images. If this is true, HRCT images could be used to distinguish precursor lesions and early (in situ) carcinomas from invasive carcinomas. Among the histologically confirmed MNGGO in our study, we could not find any AAH lesions; all lesions were BAC or adenocarcinoma except for one aspergillosis. In our study, the separate classification of PNGGO and MNGGO was helpful in the differentiation between AAH and adenocarcinoma. However, the classification did not contribute to the differentiation of BAC from adenocarcinoma. Interestingly, the grading of the internal solid portion of the MNGGO also did not contribute the differentiation of BAC from adenocarcinoma. In the three cases of proven BAC in our study, the grade of the internal solid portion on CT was 3 or 4; that is, the internal solid portion on CT exceeded 50% of the lesion.
Treatment Strategy of Mixed Nodular Grand-Glass Opacities
The potential for malignancy was very high in most MNGGOs regardless of size. To avoid resection of focal GGOs due to acute inflammation or bleeding, a three-month follow-up CT should be recommended. If the lesion remains on follow-up CT, the patient should then undergo histological confirmation. For the lesions confirmed as BAC or adenocarcinoma, the standard curative surgery such as lobectomy should be considered.
The extent of resection is somewhat controversial. Several researchers have reported, although in retrospective studies, that limited resection may be an acceptable alternative in patients with T1 N0 M0 disease and insufficient pulmonary reserve (17, 18). Recent reports have suggested that patients with no invasive lesions such as BAC or PNGGO on CT could be possible candidates for limited resection (19-21). According to five-year follow-up results in a prospective limited resection clinical trial, lung tumors 2 cm or less in diameter with HRCT findings of GGO, and without evident pleural indentations or vascular convergence may be safely managed with only limited resection (22). However, considering the probable slow-growing nature of GGO lesions, five years of follow-up is not long enough to conclude that the disease is cured. Moreover, a limited resection would be acceptable only if a BAC without an invasive component is correctly diagnosed by frozen section of the tumor. This issue must be studied in further investigations.
A critique of our study is required. First, our investigation is limited to the relatively small number of pathologically confirmed nodular GGOs and relatively short period of follow-up. Our study could be regarded as a preliminary report of long-term follow-up. Secondly, our results were not supported by statistical results. Long-term follow-up in a larger series with a prospective design will be required to elucidate the natural history of nodular GGO and to determine whether surgical intervention is acceptable or unnecessary, which may contribute to reduction of over diagnosis bias. Third, we classified and graded nodular GGO subjectively. A recently developed computerized scheme (23, 24) may help detect and characterize nodular GGOs. Fourth, serial CT scans in several individuals were performed with different reconstruction thickness in the same person. Therefore a fine structural change could have been missed.
In conclusion, MNGGOs had growth potential; most of them were pathologically adenocarcinoma or BAC. PNGGOs were stable for several months to years and most of them were AAH, BAC or focal interstitial fibrosis.
Go to :
 XML Download
XML Download