

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Generalized lymphangiomatosis is a rare disease that is characterized by a diffuse proliferation of lymphatic vessels (1). The lymphangioma is composed of lymphatic endothelium-lined cystic spaces, and this can be histologically differentiated from other vascular disorders such as cavernous or capillary hemangioma (1, 2). However, some cases of lymphangioma may be confused with other vascular disorders due to the potential overlapping histologic findings (2). Generalized lymphangiomatosis can involve any organ except the central nervous system, and the prognosis depends on the involving organ and the extent of the disease (1-3). Because radiologic examination, including CT and MR imaging, is useful for evaluating the morphologic feature as well as the extent of disease, it is important to know the radiologic findings of generalized lymphangiomatosis. In this report, we described the radiologic findings of generalized lymphangiomatosis in three patients.
CASE REPORT
Case 1
A previously healthy 4-year-old boy was admitted with respiratory difficulty three days after the onset of a fever. Chest radiograph showed widening of the superior mediastinum, cardiomegaly, bilateral pleural effusion and increased interstitial lung markings. The white blood cell count (15,000/mm3) and level of C-reactive protein (CRP) (19.8 mg/dL) were elevated, and streptococcus pneumoniae was found upon examination of the blood culture. Echocardiography revealed a large amount of pericardial effusion and an anterior mediastinal mass.
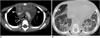
Contrast-enhanced chest CT showed a huge, bulging contoured, low density mass in the anterior mediastinum (Fig. 1A). The mass encased the thoracic great vessels and it extended from the lower neck to the retroperitoneum. The lesion extended posteriorly to envelop the trachea and the esophagus without compressing them (Fig. 1A). Pulmonary interstitial thickening and bilateral pleural effusion were also noted (Fig. 1B). There were multiple small low-density lesions in the spleen. Multiple well-defined osteolytic lesions with sclerotic margins were noted in the vertebral bodies. Chylohemopericardium and chylothorax were confirmed on the fluid analysis. Because the radiological differential diagnosis was lymphoma, incisional biopsy was performed in the lower neck. The biopsy histology was consistent with lymphangioma. After antibiotic therapy, the patient's clinical symptoms and laboratory abnormalities were improved, and he discharged from the hospital. However, the patients suffered from recurrent pleural effusion and he died six months later because of sepsis and respiratory failure.
Case 2
An 8-year-old boy was referred to our hospital as an outpatient because of incidentally detected mediastinal widening on his chest radiograph. Contrast-enhanced chest CT was performed in another hospital, and it showed a large low density, non-enhancing mass enveloping the anterior mediastinum. The lesion extended posteriorly to envelop the ascending aorta and main pulmonary artery without compressing them. Also, there were multiple low-density lesions in the spleen. Multiple well-defined osteolytic lesions with sclerotic margins were noted in the ribs, the vertebral bodies and the pelvic bone (Fig. 2A). All these lesions showed T1- and T2-prolongation on the conventional T1 and T2-weighted MR images that were obtained using a 1.5-T system (Fig. 2B). On ultrasonography, the anterior mediastinal mass was delineated as a multiseptated anechoic lesion (Fig. 2C).
Whole-body MR imaging with a short tau inversion recovery (STIR) sequence was performed for evaluating the extent of the disease. The coronal STIR images were obtained with the following parameters: TR/TE = 1600/50, inversion time = 160 msec, flip angle = 90°, slice thickness = 7 mm, number of excitation = 2 and matrix = 512×512. On the STIR MR imaging, multiple hyperintense lesions were additionally found in the pelvic bone and the upper and lower extremity bones (Fig. 2D). Based on the radiologic findings, generalized lymphangiomatosis was diagnosed without confirmation on any histological examinations. Because he had no symptoms, invasive diagnostic procedures and treatment were not performed. Follow up whole-body MR imaging that was performed after 20 months showed no significant interval change. Also, he did not complain any symptoms during the 23 months of the clinical follow up period.
Case 3
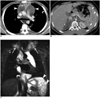
An 11-year-old boy was referred to our hospital as an outpatient because of incidentally detected mediastinal widening on a chest radiograph. CT showed a large mediastinal mass enveloping the ascending aorta and pulmonary artery. The thymus was encased within the mass and it was displaced in an anterior medial direction (Fig. 3A). The lesion extended inferiorly downward to the diaphragm. No calcification was seen within the lesion. On the non-contrast CT scan, the lesion's attenuation varied from 9 to 18 HU. There was no contrast enhancement in the lesions on the contrast enhanced CT scan. There were multiple low density lesions in the spleen. Multiple well-defined osteolytic lesions with sclerotic margin were also noted in the vertebral bodies (Fig. 3B).
On the MR images (axial & coronal T1, T2, STIR, and enhanced T1 weighted image), all the lesions showed T1- and T2-prolongation. Additional lesions were found on the STIR coronal images in the bilateral lower neck; these lesions were not clearly delineated on the CT scan (Fig. 3C). There was no contrast enhancement in the lesions on the enhanced MR images.
Generalized lymphangiomatosis was diagnosed based on only the radiologic findings. On the follow up chest CT performed 15 months after, the anterior mediastinal mass slightly increased. The lesions involving the spleen and the vertebral bodies did not show any interval change on the follow up CT. During a 45-month period of clinical follow up, the patient did not complain of any symptoms.
DISCUSSION
Lymphangioma is a rare benign neoplasm that is believed to be the result of abnormal development of the lymphatic system (1). Widespread bony and soft tissue involvement is known as generalized lymphangiomatosis or by the synonym of cystic angiomatosis (2). Generalized lymphangiomatosis forms part of a spectrum of lymphatic abnormalities, and the clinical features depend on the site and the extent of the involved organ (1-4).
Generalized lymphangiomatosis has been reported to frequently involve the bones, the mediastinum, spleen, liver, lungs, neck and pleura (1-4). Although many patients are asymptomatic, pleural involvement and osteolytic lesions can bring on respiratory difficulty and pathologic fracture, respectively. The presence of chylous pleural effusion usually indicates a poor prognosis (3, 5). The location of mediastinal involvement also affects the prognosis of the disease. Superior mediastinal lesions show a more infiltrative nature, and this may lead to a higher recurrence rate due to incomplete surgical resection (6). On rare occasions, lymphangiomatosis may display laryngeal involvement, and this causes obstruction of the airway tract (3). In our cases, the prognosis and clinical symptoms were dramatically different between case 1 and case 2/case 3. The patient of case 1 showed chylous pleural effusion and chylous pericardial effusion as an initial manifestation; he died six months after the initial diagnosis due to respiratory difficulty and sepsis. Because the site and extent of lymphangioma are important prognostic factors, performing radiologic evaluation for generalized lymphangiomatosis is crucial for planning the patient's management.
The diagnosis of generalized lymphangiomatosis should be made in association with the radiologic findings and the results of histologic examinations because the histologic findings are not always specific (2). In many cases, the lesions of lymphangiomatosis do not differ histologically from cavernous or capillary hemangioma (2). The radiologic findings of generalized lymphangiomatosis have been reported by several authors (1-4). The lesions showed as sharply defined, non-enhanced cystic lesion. In the skeletal system, multiple geographic osteolytic lesions with predominantly sclerotic borders were noted. Almost all the radiologic findings of our cases were consistent with those of the previous reports. In our reports, two of the cases (cases 2 and 3) were diagnosed as generalized lymphangiomatosis based on only the radiologic findings. Because the two patients did not have any symptoms and the radiologic findings were relatively typical, we did not performed invasive diagnostic procedures. The diagnostic value and characteristics of MR imaging for evaluating generalized lymphangiomatosis have been previously reported on, including one case that underwent whole body MR imaging (3, 7). In case 3 of our study, lymphangiomatosis in the lower neck was not found on the CT scan. Also, the lesions in the spleen and skeletal system were more clearly delineated on the MR images than on the CT scan. In case 2, the lesions in the pelvic bone and the extremity bones were additionally found on the whole body STIR MR image. Therefore, we believe that the whole body STIR MR image is very useful for evaluating the extent of generalized lymphangiomatosis.
The major differential diagnostic considerations for the children with multiple osteolytic lesions and cystic lesions involving the mediastinum and visceral organs include Langerhans' cell histiocytosis and hemangiomatosis. The osseous lesions of Langerhans' cell histiocytosis are often ill-defined and they are associated with bone marrow edema, a periosteal reaction and soft tissue enhancing lesion (8). The osseous and visceral lesions of hemangiomatosis usually show strong enhancement on the contrast enhanced CT scan (9). We think that the contrast enhanced study is mandatory for making the differential diagnosis of generalized lymphangiomatosis.
There is no specific treatment for generalized lymphangiomatosis (10). Although surgical excision is recommended for localized lymphangioma, complete excision of generalized lymphangiomatosis can be difficult or impossible. Palliative procedures often include medical therapy with interferon-alpha, draining the pleural effusions or performing pleurodesis for recurrent pleural effusions (10).
In conclusion, we reported here on three cases of generalized lymphangiomatosis. All three cases showed similar characteristic radiologic findings, but different clinical courses were demonstrated according to the extent of the disease. Whole body MR imaging with the STIR sequence showed a good capability for evaluating the extent of generalized lymphangiomatosis.

 XML Download
XML Download