

 PDF
PDF ePub
ePub Citation
Citation Print
Print



Performing resection of malignant liver tumors has been shown to increase the five-year survival rate of patients suffering with liver cancer (1, 2), but many of the patients' tumors are surgically unresectable either because of unfavorable anatomy or their poor hepatic functional reserve (3, 4). Radiofrequency ablation (RFA) is a method of local tumor ablation that destroys tumors by heating them and it offers a potential alternative therapy for unresectable primary and secondary liver tumors (5-9). Most of the clinically available electrodes, including internally cooled electrodes (6, 7), multi-tined, expandable needle electrodes (8, 9) and perfusion electrodes (10), induce coagulation necrosis in the range of 3-4 cm in diameter after only a single ablation secession. Nevertheless, clinical studies have reported on the inadequate treatment of focal liver lesions with diameters greater than 3 cm, as well as relatively high rates of marginal recurrence (11, 12). The single most important factor affecting the local tumor recurrence rate after hepatic RFA could be the ablation of a tumor-free margin of hepatic parenchyma along with the tumor itself (5, 13).
To treat liver tumors that are larger than 3.5 cm in diameter, multiple overlapping ablations are often required to create a large ablation zone encompassing the tumor and the surrounding healthy tissue rim (11, 14). However, when ultrasound guidance is used, the creation of overlapping zones of ablations in large tumors is difficult because the radiofrequency (RF) procedure almost always forms numerous microbubbles in the heated tissue. These microbubbles may obscure the unablated portions so that further electrode placement at the target site may then be difficult or impossible (14). Hence, there is a need to improve the efficacy of RFA for creating coagulation necrosis (15).
Multiple applicator approaches for RFA have recently been proposed to improve the efficacy of the RF device so as to increase the coagulation with a single application, including using multiple probe RFA in consecutive (16), simultaneous (17, 18) or switching monopolar (19-21) or bipolar (22-28) modes. A previous study by Lee et al. (25) on dual probe approaches for RFA demonstrated that bipolar RFA had better efficacy for creating larger ablation zones than did simultaneous or switching monopolar RFA. However, several prior studies have demonstrated that bipolar RFA has the limitation of creating nonspherical shaped ablation zones with short transverse diameters on the plane perpendicular to the electrode insertion axis (22, 27, 28). Theoretically, one way to overcome the limitation of the dual probe bipolar RFA is the multiple probe RFA approach where three or four electrodes are placed in triangular or square arrays with equidistant inter-electrode spacing (29). More recently, Ritz et al. (30) and Tacke et al. (31) have demonstrated that switching from bipolar RFA to using triple bipolar probes permitted the creation of large spherical shaped ablation zones for the local treatment of human liver metastases. Using the prior studies (29-31) as a reference, we assumed that multipolar RFA using triple probes, where the RF energy is applied to one electrode and then it entered to the other electrodes, could create a more spherically shaped ablation zone with a larger transverse diameter. Therefore, we evaluated the in vitro efficiency of performing multipolar RFA using triple probes for creating a large ablation zone and we compared this approach with the consecutive or simultaneous monopolar modes.
MATERIALS AND METHODS
Ex Vivo Studies
RFA Settings
RFA was performed in 15 freshly excised bovine livers that weighed an average of 7 kg each. The liver was cut into two or three 12×12×7-cm3 blocks that were immersed in a 50×20×25-cm saline-filled bath, and the bath container itself was made of acrylic plate. The RFA system used in our experiments was comprised of 17-gauge internally cooled electrodes (Valleylab; Burlington, MA) or 15-gauge perfused-cooled electrodes with a 3-cm active tip (homemade), and a 480-kHz generator (Valleylab) was used at maximum wattage. A 15×20 cm grounding pad was attached to one of the shorter width sidewalls of the rectangular acrylic bath. Three electrodes were arranged in triangular arrays with equidistant interprobe spacing of 3 to 5 cm; the electrodes themselves were placed through an acrylic plate that contained multiple holes at 5-mm intervals. The tips of the electrodes were advanced at least 4 cm into the target tissue.
We developed a perfused-cooled electrode to allow simultaneous intra-electrode cooling perfusion and interstitial saline infusion during application of the RF energy application (Fig. 1). We modified a 17-gauge cooled-tip electrode (Valleylab) with a 3-cm active tip by covering it with a 15-gauge outer sheath with a side hole for the saline infusion (Fig. 1). The outer sheath, which was made of metal and insulated, covered the shaft of the cooled-tip electrode except at its distal 3.5-cm section. The space between the 15-gauge sheath and the cooled tip electrode permitted saline infusion along the electrode. For the multiple probe applications, we used a prototype adaptor that allowed multiple probe connections; for the multipolar RF applications, we used a modified cable to connect the dispersive electrode to the generator "ground output" (Fig. 1).
Based on the results of our previously unpublished experimental study, 6% hypertonic saline (HS) was infused during the RFA at a rate of 2 mL/min through the 15-gauge perfused internally cooled electrode by using three infusion pumps (Pilotec IS; Frensenius Vial SA, Breanzins, France). A peristaltic pump (Watson-Marlow, Medford, MA) was employed with using two three-way stopcocks to infuse normal saline solution at 0℃ into the lumen of the electrodes at a rate sufficient to maintain a tip temperature of 20-25℃.
To continuously measure the local tissue temperature during the procedure, a thermocouple was inserted at 4 cm into the target tissue at the center portion of the triangle that connected each electrode. To keep the tips of the thermocouple and the three electrodes at the same depth (4 cm) in the liver, we marked the thermocouple shaft with 3 mm thick tape at 5 cm from the tip and then the distal 5 cm of the thermocouple was passed through the 10 mm thick acrylic plate.
The applied current, power output and impedance were continuously monitored by the generator during the RFA and these parameters were automatically recorded using a computer program (Real Time Graphics Software V 2.0; Valleylab). The technical aspects of RFA including the impedance and wattage changes, the tissue temperatures and the dimensions of the RF-coagulated area, were compared for each technique.
Preliminary Experiments
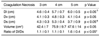
We performed preliminary experiments to find the ideal interelectrode distance for creating a spherical-shaped ablation zone for the multipolar mode with using three 15-gauge perfused-cooled electrodes. Three electrodes were placed in triangular arrays with equidistant inter-probe spacing at 3 to 5 cm through an acrylic plate that contained multiple holes at 5-mm intervals. Five separate thermal ablation zones were created at 3-cm, 4-cm and 5-cm interelectrode distances. The RF power was increased manually to 150 watts and the RF energy was applied for 20 minutes in the multipolar mode in which the current flows from one electrode to the others. Two observers working in consensus measured with calipers the long-axis diameter (Dl) and the short-axis diameter (Ds) of the central, white region of the RF-induced ablation zones at the slice that showed the maximum area. The vertical diameter (Dv) was measured by the number of slices showing discolorization. The volume of the RFA zone was evaluated by approximating the lesion to a sphere with using the following formula:π(Dv×Dl×Ds)/6. In the preliminary experiments, the short-axis diameters of RFA-induced ablation zone at 3 cm, 4 cm and 5 cm interelectrode spacings were 4.3±0.3 cm, 5.3±0.4 cm and 3.7±0.9 cm, respectively (Table 1) (p < 0.05). The largest volume of coagulation necrosis was achieved at 4 cm spacing: 42.4±7 cm3 at 3 cm spacing, 75.9±9.7cm3 at 4 cm spacing and 47.6±14 cm3 at 5 cm spacing. The volume of the ablation zone at 4 cm inter-electrode spacing was larger than that at the 3 cm or 5 cm spacing (p < 0.05) (Fig. 2). Furthermore, with the 5-cm interelectrode spacing, three of the five ablation zones were triangular with a focal defect between the two dispersive electrodes. Therefore, the short-axis diameter with the 5-cm interelectrode spacing was the shortest among the three inter-electrode spacings and the ratio of Dl/Ds (1.6) was greater than that at the 3- or 4-cm spacing (1.1). Using prior studies (20, 30) as the reference and according to our preliminary study results, a 4-cm inter-electrode distance was selected for the main experiment.
Ablation Protocol
Thirty ablation areas were created in the consecutive mode (group A, total time: 36 minutes, 12 minutes×3), in the simultaneous mode (group B, total time: 20 minutes) and in the multipolar mode (group C, total time: 20 minutes). Based on the results of the preliminary studies, the internally cooled (group A) or perfused-cooled electrodes (groups B and C) were placed in triangular arrays with equidistant inter-probe spacing at 4 cm. RF energy in the consecutive mode was consecutively applied to each of the three internally cooled electrodes for 12 minutes by changing the current flow to the second probe just after performing ablation with the first probe. In the simultaneous mode, the synchronous parallel RF energy was applied to all the perfused-cooled electrodes. For groups A and B, the RF power was manually increased to 150 watts and the RF energy was applied consecutively or simultaneously to the electrode so that current flowed from one electrode to a dispersive metallic pad, which was attached to one side wall of the saline filled bath. For the monopolar RFA, the initial impedance was controlled at 80 ohm at the placement of the electrodes in the liver. To set the impedance at 80 ohm, the liver blocks were immersed into the saline-filled bath and the distance between the electrode and the dispersive metallic pad was moved. In the multipolar mode, one electrode was used as an active electrode and it was connected to the generator RF output, and the others were used as dispersive electrodes, and they were connected to the generator "ground" output; therefore, all the current originating from one electrode entered the second and third electrodes and there was a high and constant electric field gradient between the active and dispersive electrodes. In all three groups, delivery of the RF energy was performed in the manual mode.
Lesion Size Measurement and Shape Analysis
The liver blocks containing the lesions were dissected along the plane perpendicular to the axis of the probe insertion at 5-mm intervals. As the white central area of the RF-induced ablation zone has been shown to correspond to the zone of coagulation necrosis (32, 33), two observers, who were working in consensus, measured with calipers the long-axis diameter (Dl) and the short-axis diameter (Ds) of the central, white region of the RF-induced ablation zones on the slice showing the maximum area. The vertical diameter (Dv) was measured by the number of slices showing discolorization. The volume of the RFA zone was evaluated by approximating the lesion to a sphere with using the following formula:π(Dv×Dl×Ds)/6. If the central, white regions of the RF-induced ablation zones around the electrodes were separated, then the volume of each RFA zone was calculated, respectively, and then they were summed up. In addition, the three diameters (Dl, Ds, and Dv) of the ablation zone were measured using the biggest one among the three separated ablation areas. The shape of the RF-induced ablation zone was characterized by the ratio between the long-axis diameter and the short-axis diameter (Dl/Ds).
In Vivo Study
Animal, Anesthetics and Surgical Technique
The experimental protocol was approved by the Animal Use and Care Administrative Advisory Committee of our institution. One female farm pig (weight: 50 kg) was used in this study. The animal fasted overnight, but it had free access to water before the experiments. The pig was anesthetized using an intramuscular injection of 50 mg/kg of ketamine hydrochloride (Ketamine, Yuhan, Seoul, Korea) and 5 mg/kg of xylazine (Rumpun, Bayer Korea, Ansan, Korea), and then it was prepared for RF ablation. Booster injections of up to one half of the initial dose were administered as needed. Ringer lactate solution was continuously infused during the experiment (300 mL/h). Endotracheal intubation was performed and the anesthesia was maintained using inhaled enfluorane (Gerolan; Choongwae Pharma Corporation, Seoul, Korea). Mechanical ventilation was used throughout the procedure, and the cardiac and respiratory parameters were monitored during the entire procedure period. No grounding pad was used when performing RFA in the multipolar mode.
The surgical procedure involved placing a pig in the supine position. A midline incision was done and the liver was dissected free to expose its lower two thirds. Because of the busy schedule for using the CT machines at our institute, we performed the RFA procedure with using laparotomy instead of CT guidance. After the RFA procedure, the incision was closed using nonabsorbable sutures.
Radiofrequency Procedure
To minimize potential variations in the RFA procedures, all the procedures were performed by two radiologists who had extensive experience with RF systems in their daily practice. RFA was performed using multipolar RFA, a 200 W generator (Valleylab) and three perfused-cooled electrodes. The three perfused-cooled electrodes were inserted into the liver to a depth of 35 mm at an interelectrode distance of 4 cm under intraoperative ultrasound guidance (Sonoace 5500: Medison, Seoul, Korea). RFA was performed in the multipolar mode at 150 W for 20 minutes with a 6% hypertonic saline infusion of 2 mL/min. The delivery of energy was done using an automatic impedance controlled algorithm. Three ablation zones were created in the liver.
Imaging Follow-up
A multirow detector CT scanner (Sensation 16; Siemens, Forchheim, Germany ) was used to monitor the ablations at day 4 after the RFA. The axial CT scans were obtained with 1.5 mm detector collimation, a reconstruction increment of 3 mm and a 1.3 pitch, and the scans included both lower lobes of the lung and the upper abdomen, before and after injecting 80 mL of contrast media (Ultravist 370®; Schering Korea, Seoul, Korea). The contrast media was injected at a rate of 2 mL/sec through an ear vein. The postcontrast CT scans were obtained at 60 sec after contrast administration. In addition, the sagittal reformatted images (3 mm slice thickness) were reconstructed from the CT console.
Assessment of Coagulation Necrosis (Imaging and Pathologic Studies)
The non-enhancing ablation areas in the treated liver on the contrast-enhanced CT images were measured with using Image J software (http://rsb.info.nih.gov) (34). The area and volume of the non-enhancing region were recorded for each slice. Volume was computed by integrating the area of each slice across the entire lesion.
The pig was followed up and then euthanized four days after obtaining the CT images. The livers containing the lesions were sliced in the transverse plane at 5 mm intervals. The specimens were stained for mitochondrial enzyme activity by incubating them for 30 minutes in 2% 2,3,5,-triphenyl tetrazolium chloride (TTC) (Sigma, St Louis, M0), at 20-25℃. This test is used to determine the irreversible cellular injury during the early stages of RF-induced necrosis (35). Two observers using calipers measured the two diameters (Dl and Ds) of the central, white region of the RF-induced ablation zones in the slice showing the maximal coagulation diameter. The vertical diameter (Dv) was measured by the determining the number of slices showing an unstained area.
In addition, the slices were photographed using a digital camera (Canon EOS 300D; Canon Inc, Tokyo, Japan), and the images were stored and examined with image management software (PhotoShop; Adobe, San Jose, CA). Area analysis was performed on a computer equipped with NIH Image J software. The area of coagulation on each slice was calculated using this computer program, and the volumes were calculated by multiplying the areas by the slice thickness and then they were summed to obtain the total lesion volumes. The tissues of RF-induced coagulations were fixed in 10% formalin for routine histologic processing; they were finally processed by paraffin sectioning and hematoxylin-eosin staining for light microscopic study.
Statistical Analysis
In the preliminary experiments, the shape and dimension of the ablation zones during the multipolar RFA with different interelectrode distances were compared with using a one-way analysis of variance (ANOVA) test, and this was followed by a Bonferroni post-Hoc test for group to group comparisons. The dimensions of the thermal ablation area and the technical parameters of the three groups (consecutive vs. simultaneous vs. multipolar modes) were compared using the ANOVA test. Repeated measures of ANOVA were performed to compare the tissue temperature at the center portion of the inserted electrodes. For all the statistical analyses, a p value less than 0.05 was considered statistically significant. The statistics were performed using SPSS 9.0 computer software (SPSS Inc., Chicago, IL).
RESULTS
Ex Vivo Experiment
Technical Parameters
Mean initial tissue impedance before RFA was set at 80 Ω with three electrode placements. Although the impedance was not severely changed after starting the RF application in the simultaneous mode, it was increased to 90-110Ω in the consecutive mode because of the difference in the surface area of the active portion of the probes (only one of three electrodes was used for RF energy application). In addition, in the simultaneous and multipolar modes, the impedance was gradually decreased during RFA, whereas in the consecutive mode, the impedance was markedly increased 3-5 minutes after starting RFA; this induced a significant decrease of current flow during the procedure. The mean current flow during RFA was 937.5±398 mA, it was 2,010±57 mA in the simultaneous mode and 1,824±189 mA in the multipolar mode. The differences in the mean current flow between the consecutive and simultaneous modes and between the consecutive and multipolar modes were statistically significant (p < 0.05).
Lesion Size Measurement and Shape Analysis
The consecutive mode generated three separate ablation spheres, but the simultaneous or multipolar modes generated unified ablation zones along the three electrodes. The maximum long-axis diameters (Dl) of the RF-induced central white zones that were measured in the gross specimens of the three groups were as follows: 2.7±0.1 cm in group A, 5.7±0.7 cm in group B and 5.7±0.5 cm in group C (p < 0.05) (Table 2). The mean vertical diameters (Dv) along the axis of the electrodes were 3.8±0.4 cm in group A, 3.8±0.4 cm in group B and 5.0±0.4 cm in group C (p > 0.05) (Fig. 3). In addition, the mean short-axis diameters (Ds) of the ablated spheres in groups A, B and C were 2.4±0.2 cm, 3.5±1.0 cm and 5.2±0.3 cm, respectively (p < 0.05). The difference in the short-axis diameter for each group was statistically significant.
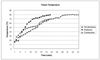
Compared with the simultaneous mode, the multipolar mode tended to produce round-shaped coagulation with a less prominent "waist" formation between the electrodes, i.e. the ratio of Dl/Dv was 1.6±0.4 in group B and it was 1.1±0.1 in group C (p < 0.05). There was a statistically significant difference in the Dl/Ds between groups B and C. Furthermore, the volumes of the ablation zones obtained with the consecutive, simultaneous and multipolar modes were 37.6±4 cm3, 44.9±12.7 cm3 and 78.9±6.9 cm3, respectively, and the differences in the volume of the ablation zones between the consecutive and multipolar modes or between the simultaneous and multipolar modes were statistically significant (p < 0.05). The graphs in Fig. 4 show the mean temperature at the center portion of the inserted electrodes. In groups A, B and C, the mean final-temperature values were 80±10℃, 69±18℃ and 79±12℃, respectively (p < 0.05)
In Vivo Experiments
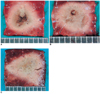
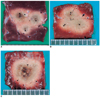
The pig tolerated the RFA procedure very well, and no major complications occurred during the follow-up period. As was observed ex-vivo, the in vivo impedance values during multipolar RFA varied within the range 50Ω to 100Ω (mean: 57±9Ω), and the impedance was well controlled to < 60Ω. The RFA regions created in the entire treated liver exhibited a characteristic central white zone surrounded by a red hemorrhagic zone. After staining with 2% 2,3,5-triphenyl tetrazolium chloride, the normal liver parenchyma appeared pink, but the central white zone was unstained (Fig. 5). The mean values of D1, Dv and Ds in the central white zones of the ablated regions were 6.5±0.2 cm, 4.8±0.8 cm and 3.7±0.8 cm, respectively, and the mean volume of the non-enhancing zones induced by multipolar RFA was 60.5±17.9 cm3 (Table 3). All the ablated zones on contrast-enhanced CT scans obtained 4 days after the RFA demonstrated non-enhanced, hypo-attenuated regions (Fig. 5). The mean volume of the non-enhancing zones induced by multipolar RFA was 65.7±17.9 cm3. There was no significant difference between the values measured on the gross specimen and on CT (p > 0.05).
Histopathologically, the ablated regions in representative cases demonstrated a central necrotic zone surrounded by a peripheral hemorrhagic zone that consisted of necrotic hepatocytes, interstitial hemorrhage and polymorphonuclear leukocyte infiltrates. No viable cells were found within the central necrotic zone, but within hemorrhagic lesions, there were areas of sinusoidal congestion and hemorrhage that were accompanied by advanced necrotic changes and patches of living cells.
DISCUSSION
Some recent investigations have introduced the use of multiple RF probes as a strategy to increase the dimension of the spherically shaped ablation regions (29, 30, 31, 36). Multiple probes (two or more) can be utilized to deliver RF energy in several FRA modes: the consecutive monopolar, simultaneous monopolar, switching monopolar, switching bipolar and multipolar modes (25, 27, 29, 30). The consecutive mode applies energy continuously to one electrode after the other in a monopolar fashion, and this approach requires a long procedure time. The simultaneous mode is the synchronous application of energy to all electrodes. In this mode the maximal energy of any electrode is reduced in relation to the number of electrodes that are used (Ohm's law). When using the monopolar mode, RF power is applied to only a single electrode at a time. This approach takes advantage of avoiding electrical interactions between multiple electrodes. The switching bipolar mode applies RF energy to one electrode and the other electrode is used as a return electrode, like the bipolar mode, but all the possible electrode pairs of the multiple electrodes are activated automatically, one after the other, for a short period of time (30, 31). In the multipolar mode, RF current is passed through one electrode and the other two electrodes are used as the return electrodes. Previous investigations (26, 30, 31) have demonstrated that bipolar or switching bipolar RFA show greater energy efficiency than monopolar RFA. However, these studies encountered the problem of a rapid rise in impedance that was related to too much condensed current between the electrodes. In order to avoid the problem of a rapid rise in impedance during multipolar RFA, we used HS infusion during the RF energy delivery to decrease the rise in impedance by increasing the electrical and thermal conductivity (25, 26).
In our study, the multipolar mode showed the best results for creating larger ablation areas. Larger ablation zones were created using the multipolar mode compared to either the consecutive or the simultaneous monopolar modes. This finding could be due to several factors. First, this could be related to the greater energy efficiency of the multipolar mode where the current is condensed between the electrodes (22-24). In the simultaneous mode, the current preferentially travels away from the probes rather than between them because of the electric shielding of the probes, which is similar to the Faraday Cage Effect (19, 20, 29, 31). Therefore, very little tissue heating takes place between the probes that are activated at the same voltage (19-21). Furthermore, the maximal energy of any electrode is reduced in relation to the number of electrodes used (Ohm's law): if three electrodes are used with a 150 W generator, 50 W would be the maximum power deliverable to each electrode. By contrast, for the multipolar mode, the current is preferentially deposited to the area immediately surrounding the electrodes and so high current densities may be expected if the maximal power output is delivered from the RF generator. Second, the findings for the multipolar mode may be related to heat trapping between the electrodes. In the consecutive mode, heat is diverted from the ablation site in all directions. In the multipolar mode, one electrode is thermally shielded by the opposing second and third electrodes so that they actively heat the tissue in their proximity (22-25). Furthermore, as the heat is trapped between the two electrodes and higher temperatures are achieved, there is less cooling in the direction of the collateral electrode than is the case with monopolar ablation.
There have been three previous studies regarding multiple probe RFA that have used more than two probes (20, 30, 31). Two of the previous studies used switching bipolar RFA with triple bipolar electrodes (they described it as multipolar RFA), and this technique could successfully treat 4-5 cm metastatic liver tumors. However, they did not describe the size of the ablation region that could be achieved after a single application of RF energy in the switching bipolar mode; therefore, direct comparison with our study is not possible. Haemmerich et al. (20) have demonstrated that a rapid switching RF application with triple cluster electrodes could create larger ablation zones than a simultaneous RF application can with using the same time period: 116.4 cm3 with a rapid switching mode vs. 22.3 cm3 with a simultaneous mode. In addition, the rapid switching RFA for 12 minutes created a similar ablation volume as compared to a sequential method for 36 minutes. This improved efficiency of the rapid switching mode compared to the simultaneous mode could be attributed to the simultaneous application of power to multiple RF electrodes, which is fundamentally limited by the electrical interactions that limit heating between electrodes, as well as the thermal shielding effect of the probes from vascular mediated cooling (19, 20). The ablation volume of the rapid switching RFA with using triple cluster electrodes (116.4 cm3) was much larger than that of the multipolar RFA in our study (79 cm3). However, in the previous study, the researchers measured the RF-induced discolored area as an ablation region. However, in our study, we measured the central white zone of the RF-induced discolored area as an ablation region, according to the recommendations of International Working Group on Image-Guided Tumor Ablation (37). Considering that the peripheral pinkish zones of the ablation regions were 1cm thick, if we measured the RF-induced discolored area as an ablation region, the multipolar RFA-induced ablation volume could be much larger than that of the rapid switching RFA, which the same as was noted in the previous study. Furthermore, compared to the multipolar RFA that does not need ground pads, it is possible that patients could be at higher risk for burns with the multiple probe system. The alternating monopolar RF mode with multiple probes may increase the ground pad temperature compared to standard RFA with a single probe. That is because there is a more continuous deposition of RF power into the subject without any interval cooling; this is possible in alternating monopolar RFA when compared to the standard monopolar RFA.
Our study results suggest that when treating large tumors, the proposed multipolar RFA using triple probes with HS infusion may destroy tumors with a single application and with a reduced treatment time. Although placing three probes into the target tumor can make the RFA procedure difficult, it is only minimally more complicated compared to the insertion of a single probe. Furthermore, inserting the probes before starting the RF energy instillation may avoid the difficulty of moving the probe from one site to another. RF technology with a single RF electrode creates multiple overlapping or consecutive zones of ablation, and it greatly increases the treatment time, the anesthetic risks and the treatment costs. A multipolar approach would be able to overcome these limitations. Furthermore, the multipolar RFA with multiple probes in our study created a spherical-shaped ablation zone that is better suited for tumor ablation than overlapping monopolar RFA. Creating spherical ablation zones could be valuable in the clinical application of RFA for liver tumors as focal liver lesions are usually round or oval-shaped.
Multipolar RFA using cooled-wet electrodes has certain drawbacks. First, all the current originating from one electrode must also enter the second and third electrodes (25). When the degree of cooling at the site of each electrode is different due to differences in perfusion, one electrode reaches a higher temperature than the other, which can lead to boiling and a rapid rise in impedance. Second, since the current flows between the electrodes when using the multipolar mode in a perfused organ, this will likely result in minimal thermal lesion formation that is outside of the center of the triangle because of the lack of current density directed 360 degrees around each needle. This could be a potential disadvantage of the multipolar mode. Third, the multiple probe RFA technique has a higher cost than the single consecutive RF application. Fourth, when using multipolar RFA, the probes must ideally be placed equidistant from each other. In the clinical environment, the insertion of three probes equidistant from each other might be difficult. If the probes are not precisely placed, the current could flow to the nearest portion of the exposed ground probe, resulting in a bizarrely shaped thermal ablation area. Last, multipolar RFA with HS infusion has the concern for an irregular shape of the coagulation necrosis due to the uneven distribution of injected HS, as was reported previously (38, 39).
Our experimental study has certain limitations. First, the application of our study results to human liver tumor is limited because our study was performed on normal liver parenchyma. The tumor heterogeneity and the heat sink effect by the tumor vessels may modify the results that we observed (40). However, despite these concerns, our model provides a reliable basis for a comparative study on the efficiency of different RF modes. Second, we did not perform the rapid switching mode RFA due to lack of an effective electromechanical switch that could control the triple electrodes in real time. Further, a comparative study between the rapid switching mode and the multipolar mode is needed. Third, tissue temperature was measured at only one point, i.e. midway between the three electrodes. The 3-D temperature distribution could have been obtained if we had measured the tissue temperature at many points. Fourth, even though multipolar RFA using multiple probes showed a better performance in creating large ablation zones when compared to monopolar RFA, the placement of three probes through the intercostal spaces may present technical difficulties in the clinical setting. Therefore, our study results may represent the clinical scenario of intraoperative RFA, and the results could be extrapolated to intraoperative RFA rather than percutaneous RFA. Last, even though the animal well tolerated the multipolar RFA procedure without any major complications, the number of in vivo experiments (three RFA lesions in one animal) is too small to definitely prove the safety of multipolar RFA. Therefore, to resolve any possible safety issues, an experimental study with a large animal tumor model of a clinically relevant size is necessary before this procedure can be clinically applied to the treatment of human liver malignancies.
In conclusion, multipolar RFA with HS infusion using perfused-cooled electrodes shows the capability to create a larger zone of thermal coagulation than can simultaneous monopolar ablation. We believe that the increased volume of coagulation necrosis created by multipolar RFA, if it is reproducible in tumors, would be of significant clinical benefit.




 XML Download
XML Download