

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Since the first successful aortoiliac angioplasty was done in 1980 (1-3), and with the appearance of vascular stents in the late 1980s, angioplasty and/or stent placement has provided new therapeutic options for the treatment of chronic aortoiliac occlusive disease.
However, according to several reports, performing only percutaneous transluminal angioplasty (PTA) for irregular, eccentric, long, ulcerated stenoses and occlusions has demonstrated unsatisfactory long-term patency rates (4-7).
Endovascular stenting for iliac arterial occlusive disease has recently shown some good results and this technique has become widely accepted as a primary treatment for iliac arterial occlusive disease (8-11). The long-term clinical results of iliac arterial stenting are important baseline factors for determining the therapeutic options and there have been several reports concerning the 5-year follow up results of iliac arterial stent placement. However, in spite of the various clinical studies, the 10-year survey data is still somewhat limited (12) and any report concerning 10 years experience at a single Asian institution is rare.
The purpose of our study was to evaluate the long-term therapeutic results of iliac arterial stent placement by conducting a retrospective review of a 10-year period in a single institution.
MATERIALS AND METHODS
Patient population and stent placement
A total of 206 patients who underwent iliac arterial stent placement from May, 1994 to April, 2004 were retrospectively evaluated for their long-term stent patency. One hundred ninty-eight patients were male and eight were female (the ages ranged from 48 to 84 years, mean age: 64 years).
No absolute exclusion criteria were used other than a patient's refusal to participate in our study. The patients who were proven to have iliac arterial occlusive disease on Doppler ultrasonography, CT angiography or by the low ankle brachial index (ABI) were the candidates for stent insertion and most of these patients wanted to avoid the surgical risk and comorbidities.
We performed primary stenting as a baseline treatment strategy unless there was an absolute demand for only angioplasty from the patients and/or the clinical department. The policy of primary stenting was based on the reports by Vorwerk and Nawaz (13, 14). However, the finding of more than 30% residual stenosis after repeated angioplasty or a flow limiting dissection was also used as additional criteria for stenting.
Informed consents were obtained from all the patients or from their legally responsible guardian. 195 patients (95%) underwent stent placement in an angiographic clinic under local anesthesia and 11 patients underwent intraoperative stent placement. The procedure for primary stenting included the placement of a 7 F introducer sheath ipsilaterally, and then a 0.035-inch guide wire (Glidewire, Terumo, Tokyo, Japan), was passed through the stenotic segment. The stent was subsequently placed over the guide wire to completely cover the stenotic segment. If this failed, an antegrade approach to stenting was attempted with using the contralateral common femoral artery (CFA). Fluoroscopic "road maps" were used to precisely place the stent. The diameters of the stents we used were measured from the normal proximal or distal segments on either side of the stenoses and also from the contralateral corresponding artery. After deployment, the self-expandable stents were routinely dilated with using a balloon catheter that had a diameter from 6 mm to 10 mm. Poststent angiographic images were obtained with the bilateral oblique view and the anterior-to-posterior view. All the patients were given an intravenous bolus of 80 IU/kg heparin during their procedures. During the initial period of study, the administered medications after the procedure included asprin (500 mg per day) and dipyridamole (225 mg per day for 3-6 months). During the midterm study period, aspirin (325 mg per day) and ticlopidine (100 mg 1T b.i.d. for 3-6 months) was used for the post-stent medication. After Feb. 2000, the post-stent medication was changed to aspirin (100 mg per day) and clopidogrel (75 mg per day for 3-6 months).
The decision of which stent to use was left to the discretion of the operator, but balloon-expandable stents were usually deployed for the focal or short segmental lesions, and self-expandable stents were deployed for the long segmental or diffuse lesions. Various types of stent were used. The original Palmaz, Palmaz Corinthian, Palmaz GENESIS stent (Cordis Europa N.V., Johnson & Johnson's Corp, The Netherlands), and the EXPRESS LD stent (Boston Scientific, MA, USA) were the balloon expandable stents that were used. The self-expandable stents included the Wallstent (Schneider, Boston scientific, MA, USA), the Niti-S stent (Taewoong Medical, Seoul, Korea), the SMART stent (Johnson & Johnson's Cordis Corp, Miami Lakes, FL), and the Symphony stent (Boston Scientific vascular, Natick, MA).
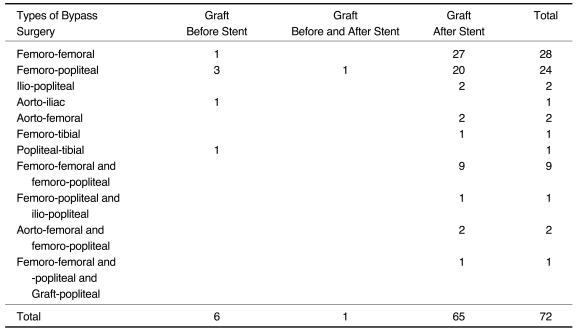
Combined bypass graft surgery was performed in 72 of 203 (35%) patients (Table 1) (Fig. 1). Six patients underwent bypass surgery before their stenting and the stent was inserted for the additional newly developed iliac lesions. Sixty-five patients underwent bypass surgery after their stent insertion. When the stent was placed prior to bypass surgery, the subsequent bypass surgery was performed within one hospital stay. One patient had an occluded femoropopliteal bypass graft before their stent insertion. Therefore, this patient underwent another femoropopliteal bypass after placement of the stent. For the patients with coexisting contralateral long segmental obstruction of the common and external iliac arteries, we performed ipsilateral stent placement and subsequent crossfemoral bypass surgery. For the patients with bilateral diffuse iliac arterial disease or for the patients with poor distal run off vessels, a combination of bypass surgery such as aortofemoral or femoropopliteral bypass surgery was performed before or after stent placement.
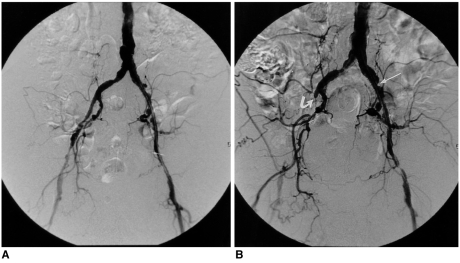
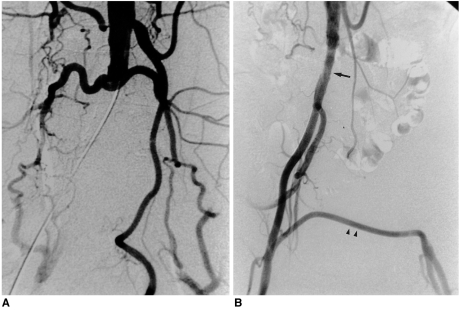 | Fig. 1
A. A 64-year-old male patient shows complete obstruction of both the common iliac artery and the external iliac artery. This patient underwent stent placement at the right common iliac artery and the external iliac artery with subsequent femorofemoral bypass graft surgery.
B. The 48 month follow up arteriography shows the well preserved patency of the stent at the right common iliac artery and the external iliac artery (arrow) and the femorofemoral bypass graft (arrowheads).
|
Data Analysis and Study Endpoints
The sites of the lesions were recorded from the common iliac artery (CIA) to the external iliac artery (EIA). The patients having lesions at both the CIA and EIA were also described. The shapes and distribution of the lesions were recorded under the categorization of focal stenosis, segmental stenosis, multifocal or diffuse stenosis, and complete obstruction. Focal stenosis was defined as a localized, flow limiting stenosis that was less than 1 cm in total length. Those lesions having a measurable distance or if there were more than two continuous lesions that consisted of narrowed segments, then they were considered as segmental lesions. Multifocal or diffuse stenosis was indicated by the presence of more than two separated flow limiting stenotic lesions in a tandem location or by the presence of bilateral diffuse disease.
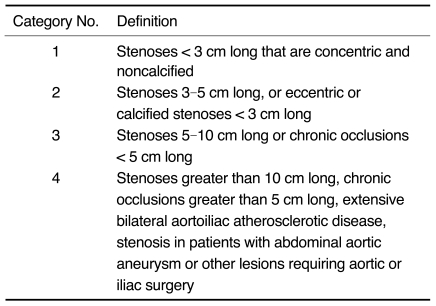
The lesion lengths were recorded in each lesion from the baseline angiographic images and they were classified into four categories; lesions less than 3 cm, 3-5 cm, 6-9 cm and then lesions equal to or greater than 10 cm in length. For the patients having multifocal or diffuse stenosis, the distance from the most proximal stenosis to the most distal stenosis was considered as the total length of the lesion. The lesion's lengths were categorized according to the criteria of the Society of Cardiovascular and Interventional Radiology (SCVIR) (Table 2), and all the patients were grouped into the four classes of the SCVIR classification (11).
The status of the femoral runoff vessels was scored for each limb according to the Society of Vascular Surgery/International Society of Cardiovascular Surgery (SVS/ISCVS) grading system (Table 3) (15). For the patients who did not undergo bypass surgery, the pre-stent angiographic images were used for grading the run off scores. However, a coexisting patent ipsilateral femoropopliteal bypass graft was considered as a patent superficial femoral artery (SFA). In addition, the patient who underwent prestenting and/or poststenting bypass surgery was also considered as having patent distal run off vessels. If contralateral iliac stenting was performed along with femorofemoral bypass surgery, then the run-off score was based on the ipsilateral lesion site limb.
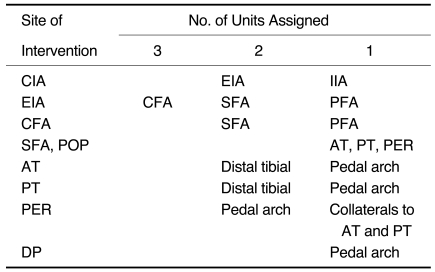
Table 3
Weighting of the Runoff Vessels
Note.-CIA = common iliac artery, EIA = external iliac artery, IIA = internal iliac artery, CFA = common femoral artery, SFA = superficial femoral artery, POP = popliteal artery, PFA = profunda femoral artery, AT= anterior tibial artery, PT = posterior tibial artery, PER = peroneal artery, DP = dorsalis pedis artery
*Points assigned for degree of occlusion: 3 = occluded throughout most of its length; 2.5 = occluded for less than half its length with visible collaterals; 2 = 50%-99% stenosed;1 = 20-49% stenosed; 0 = normal or minimal evidence of disease (ie, less than 20% narrowing)
![]()
Immediate poststent technical success was defined when there was less than 30% residual stenosis, restoration of a rapid antegrade flow was noted angiographically, and/or there was less than a 10 mmHg resting transstenotic mean pressure gradient on the homodynamic 'pull-back' measurement with using a single transducer.
For a vessel to be considered patent during follow-up, a treated limb had to meet the study's clinical criteria (no intervening percutaneous or surgical intervention involving the iliac artery, and no deterioration in the clinical status), the noninvasive criteria (an ABI maintained within 15% of the maximum post-stenting value or there was no evidence of restenosis on the color Doppler US), and when it was performed, the angiographic criteria (no evidence of restenosis). Restenosis was defined as more than a 30% reduction of diameter inside or at the ends of the stents, as noted on the CT angiography or on the digital subtraction angiography, and/or a greater than 2.5 peak systolic velocity ratio on the color duplex ultrasonography. Limbs that violated any of these criteria were considered to be occluded for the purposes of the analysis.
The symptoms and clinical severity of the lower extremity ischemia were classified and followed by using the Fontaine classification (Table 4) (8). The definition of the patency was consistent with the reporting guidelines suggested by Sacks (15).
Follow up of stent patency was performed with using both the medical imaging and the clinical assessment. The imaging modalities included conventional angiography, CT angiography and/or color Doppler ultrasonography. The clinical assessment consisted of the ABI, symptomatic evaluation and the physical examination. The follow up intervals were somewhat irregular before Feb. 1999, but since then, the immediate postprocedural measurement of the ABI was followed up at 3 month, 6 month, 12 month and at each following year. Conventional angiography was indicated when the color Doppler sonography and/or ABI suggested the presence of in-stent restenosis or obstruction. A decrease of more than 15% of the post-stent maximum ABI was regarded as stent failure. CT angiography was mainly recommended for those patients who maintained uninterrupted patency for more than 12 months of follow up. CT angiography was performed at a six month or one year interval at the outpatient clinic, according to the decision of the physician.
The follow up data was collected by reviewing the medical records and by interpreting the follow up medical images. When the imaging follow-up result was not available, the results of a physical and the symptomatic evaluation done at the outpatient department were used for determining patency. For the cases that were lacking the outpatient clinical examination data, telephone interviews were performed for evaluating the clinical symptoms, the life quality and the interval changes or the degree of the present claudication as compared with the immediate post-stent period.
The cardiovascular risk factors were recorded; these were based on the medical records and they included diabetes, smoking and hypertension.
Statistical Analysis
The basic unit of analysis was the limb and not the patient. The time of the primary patency of the stent was calculated by performing a survival analysis with the Kaplan-Meier method.
Because only six of the 206 patients (0.03%) were female in this study, gender was excluded from the statistical analysis. Age, stent type and diameter, the lesion site, lesion shape, lesion length, the SCVIR classification, the total run off scores, the Fontaine classification and the cardiovascular risk factors (diabetes mellitus: DM, hypertonsim: HT and smoking) were analyzed with the Breslow test to screen for variables that affected the primary patency of the stent.
All the factors included in the Breslow test were evaluated for their relationship with stent patency by using the Cox proportional hazards test to compensate and adjust for the effect of each predictor variable.
The pre-stent ABI and the post-stent ABI, the transstenotic pressure gradients and the changes of the Fontaine classification were compared by using paired t tests.
Go to : 
RESULTS
Two hundred eighty-four stents were placed in 249 limbs of 203 patients. In four limbs of three patients, the procedure failed due to the failure of the guide wire to pass across the lesion. The immediate technical success rate was 98% (203/206). Single limb treatment was performed in 157 patients (77%) and bilateral stent placement was performed in 46 patients (23%). Eleven patients underwent intraoperative stent placement.
The number of balloon expandable stents placed was 54 Palmaz stents and three EXPRESS LD stents. The number of self-expandable stent placed was as follows; Wallstent (n = 106), Niti-S stent (n = 5), SMART stent (n = 114), and the Symphony stent (n = 2). The stent diameter ranged from 6 mm to 14 mm, and the number of stents used was: 6 mm (n = 4), 7 mm (n = 19), 8 mm (n = 139), 9 mm (n = 42), 10 mm (n = 74), 12 mm (n = 5), and 14 mm (n = 1).
Lesions were identified in the CIA (n = 95), the EIA (n = 106), and both the common and external iliac arteries (n = 48). The shapes of the lesion were 106 focal stenoses, 82 segmental stenoses, 21 multifocal or diffuse stenoses, and 40 limbs with complete obstruction. The number of lesions in each category of the lesions' length was: below 3 cm (n = 125), 3-5 cm (n = 62), 6-9 cm (n = 44), and more than 10 cm (n = 18).
According to the classification of the SCVIR, 51 lesions (20%) were category 1, 86 (35%) lesions were category 2, 72 lesions (29%) were category 3, and 40 lesions (16%) were category 4.
Eighty limbs (32%) showed a flow limiting stenosis or obstruction at the SFA, and eight limbs had lesions in the CFA. Compromise of the profunda femoral artery (PFA) was seen in 10 limbs. The mean value of the total run off score was 0.9±1.8.
The pre- and post-stent ABI records were available in 74 limbs of 62 patients and the mean ABI value was increased from 0.7#x00B1;0.2 before stent placement to 0.9±0.1 after stent placement. For the other patients who lacked a prestent ABI value, follow up of the ABI was also performed. Improvement of the ABI after stent placement showed statistically significant changes on a paired t test (p = 0.02).
The mean transstenotic pressure gradients were available for 84 patients. The mean pressure gradient decreased from 21.3±15.6 mmHg to 1.3±5.4 mmHg before and after stent placement, respectively. The pressure gradients also showed statistically significant improvement on paired t tests (p = 0.00).
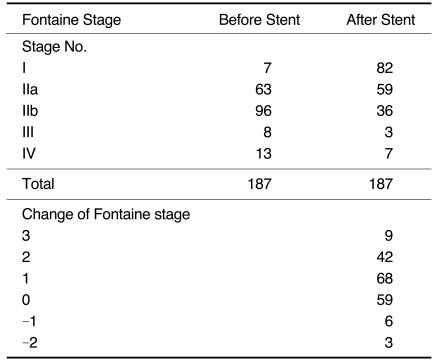
One hundred eighty-seven patients had a pre- and post-stent Fontaine classification. The median value of the Fontaine classification changed from 3 to 2 before and after stent placement, respectively. The changes of the Fontaine classification before and after treatment are shown in Table 5 and there was statistically significant improvement of the Fontaine stage on paired t tests (p = 0.00).
Nine patients expired during the follow up periods. The causes of death were gastrointestinal bleeding for one patient, myocardial infarction in three patients, diabetic nephropathy in two patients, sepsis associated with chronic renal failure in two patients and hepatocellular carcinoma in one patient.
The lengths of the follow up periods ranged from one month to 120 months (mean: 31±25.2 months). Doppler ultrasonography was performed in all the patients during the follow up periods according to the follow up protocol. Thirty-one conventional angiographies were performed in 30 patients, and CT angiography was performed in 49 patients. Determination of the final stent patency was based on Doppler sonography in 70 patients, ABI in 36 patients, CT angiography in 29 patients, conventional angiography in 19 patients and by a clinical decision with a phone call and/or a physical examination for 49 patients.
Overall, complications occurred in 12 of the 203 patients (6%). Major complications that required further management were seen in six of the 203 patients (3%). One patient who underwent common iliac artery stent placement showed acute thrombotic occlusion of the common femoral artery within 24 hours after the stent placement. The occluded common femoral artery was treated with thrombolysis. The balloon or stent associated dissections were treated by the additional placement of stents in three patients. Overlay of the stent upper margin on the contralateral common iliac orifice occurred in two patients, and so additional stent placement was performed in the contralateral common iliac artery.
Minor complications that were treated with conservative management and/or medical management were seen in six of the 203 patients (3%). Four patients with distal embolic occlusion of the infrapopliteal small branch vessel improved on the clinical follow-up with instituting anticoagulation therapy only. Hemodynamically insignificant small antegrade dissections associated with the stent were seen in three patients, and these were left alone without further management.
One hundred seventy-seven of the 203 patients (87%) maintained uninterrupted stent patency until the final follow-up (Fig. 2). 26 of the 203 (13%) patients presented with stenosis or obstruction of their stents on the follow up imaging studies. Secondary intervention was performed in a total of thirteen patients. Eleven patients were continuously followed up thereafter, but the follow up data was not available for two patients after they underwent secondary intervention. Restenosed stents were left without further intervention in nine patients. Subsequent bypass surgery was performed in four patients who were identified as having stent obstruction.
 | Fig. 2A 68-year-old male patient underwent left common iliac artery and external iliac artery stent placement on October 1994. The patient had a completely occluded right femoropopliteal bypass graft.
A. The angiograms obtained 5-years after stent placement show the well preserved stent patency without any hemodynamically significant stenosis.
B. Follow-up angiography performed on March 2003 (101 months from the initial stent placement) also shows the good instent flow without significant stenosis. Note the minimal progression of the eccentric stenosis (arrow) at the proximal portion of the stent, but this is hemodynamically insignificant. Newly developed occlusion of right external iliac artery can be seen (curved arrow).
|
The cardiovascular risk factors were diabetes in 74 patients (36%), hypertension in 126 patients (62%), and smoking in 151 patients (74%).
Statistical analysis and the predictors of outcome
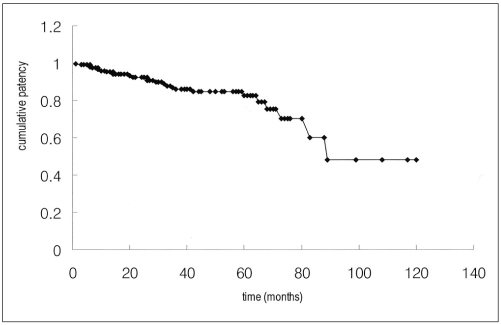
The cumulative primary patency rates with their confidence intervals (CI) and standard errors (SE) for the iliac arterial stent placement at 3, 5, 7 and 10 years were 87% (95% CI: 0.81-0.92, SE: 0.03), 83% (95% CI: 0.76-0.90, SE: 0.04), 61% (95% CI: 0.39-0.84, SE: 0.11), and 49% (95% CI: 0.21-0.77, SE: 0.14), respectively (Fig. 3).
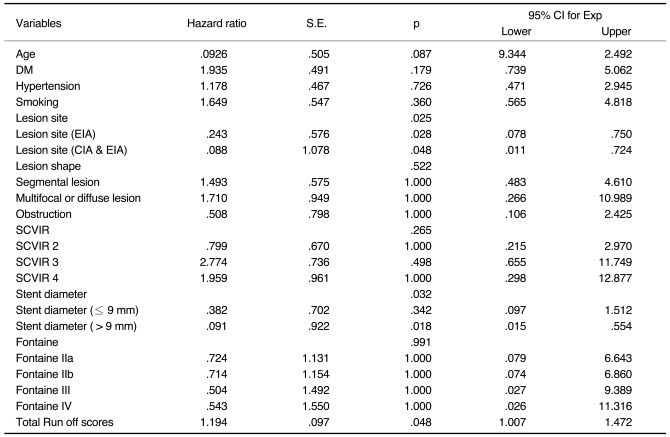
Age, the stent type and diameter, lesion site, lesion shape, SCVIR classification, the total run off scores, the Fontaine classification and the cardiovascular risk factors (DM, HT, smoking) were analyzed with using Breslow tests to screen for variables that affected the primary patency of the stent, but none of these variables showed a statistically significant relationship with the primary stent patency. Except for the stent type and the lesion length that were excluded from the Cox regression analysis because one of the frequencies of these subcategory was too small for analysis, all the other variables in the Breslow test were included in the multivariate Cox regression model.
According to the occlusion hazard rate analysis with using Cox regression testing, with the assumption that the other variables are constant, the lesion site (p = 0.025), the stent diameter (p = 0.032), and the run off score (p = 0.048) showed to have a statistically significant influence on the primary stent patency (Table 6). When the iliac lesions were located at the EIA, the occlusion hazard rate was 24% higher than in the cases having CIA lesion only (p = 0.03). For the patients having lesions at both the CIA and EIA, the occlusion hazard rate was 9% times higher than for the cases with CIA lesion (p = 0.048). Stents having the same or larger diameter than 10 mm showed 9% higher occlusion hazard rate than a stent with a diameter less than 10 mm (p = 0.02). However, the group having a stent with a diameter less than 8 mm or the group having a stent 8 mm or 9 mm in diameter showed no statistically significant difference between the occlusion hazard rate (p = 0.02). With increasing the run off scores by one point, the occlusion hazard rate was increased 1.194 times (p = 0.048). The lesion shape, SCVIR classification, cardiovascular risk factors (DM, HT, smoking) and Fontaine classification showed no statistically significant influence on stent patency.
Comparison of the ABI (p = 0.02), the Fontaine classification (p = 0.00), and the transstenotic pressure gradients (p = 0.00) before and after stent placement showed statistically significant improvement on the paired t test.
Go to :
DISCUSSION
In spite of the good long-term patency that's been observed for surgical bypass grafting, the surgical management of aortoiliac insufficiency in the patients with intermittent claudication has been discouraged because of the risks associated with the aortoiliac bypass surgery. According to the surgical experiences of six large series that involved 1,270 patients who were treated for claudication and limb-threatening ischemia, the weighted surgical mortality was 4%, and major complications were seen in 21% of the cases (16-20). The complications of aortoiliac bypass surgery are significant and they include myocardial infarction, congestive heart failure, multisystem organ failure, stroke, spinal cord ischemia, intestinal infarction, aortoenteric fistula, acute renal failure and respiratory failure.
Balloon angioplasty represents a less invasive therapeutic option for the treatment of patients with aortoiliac insufficiency, and it has been demonstrated to have acceptable associated risk for the patients suffering with intermittent claudication. As a consequence, balloon angioplasty remains the gold standard for the percutaneous treatment of aortoiliac stenosis (21). Becker et al. analyzed 2,697 procedures and they found an average technical success rate of 92%, a 2-year patency rate of 81% and a 5-year patency rate of 72% (7). Although these results are quite satisfactory, the complications and limitations associated with PTA have caused interventional radiologists to search for new approaches that can provide better patency for the diseased vessel with smooth contours (4, 22, 23).
The placement of metallic vascular end prosthesis was first used in interventional radiology more than 10 years ago, and numerous reports have been published on this technique's success (9, 12, 13, 24). Since their first applications by Dotter, endovascular metallic stent placement has been widely used for the treatment of aortoiliac occlusive disease (7, 25, 26). Lesions that respond poorly to PTA, such as complex calcified or eccentric stenoses, plaques with ulceration or aneurysm formation, long segmental stenoses with an irregular surface and also chronic occlusions are the ones that are well indicated for stent placement (23, 27, 28).
In our study, the primary patency rates for all the limbs, as determined by Kaplan-Meier analysis at 3, 5, 7, and 10 years, were 87%, 83%, 61% and 49%, respectively. The patency rates of this study were relatively similar to those reported by Schürmann, who reported a patency rate of 83% for 5 years with self-expandable stent placement in 110 patients (12). Vorwerk et al. reported a 4-year patency rate of 78% and 82% for the primary and secondary stenting procedures, respectively, in 100 patients (13, 28). Cikrit and colleagues reported a 5-year patency rate of 63% in 38 limbs that were treated by Palmaz stent placement, whereas Palmaz et al. initially reported a 92% patency rate at 9 months (29). Primary 4-year patency rates as high as 86% have been recently reported (7, 30). The presumptive 7-year and 10-year patency rates in our study showed a wide confidence interval (0.39-0.84 and 0.21-0.77, respectively), which wase not statistically guaranteed for making comparison with the data of the previous studies. De Vries and Hunink reported that the 5 year patency rates for the patients treated with aortoiliac bypass surgery were 91% for the patients with claudication and 87.5% for the patients with ischemia (31). As with our series and Schürmann's series, the 5-year patency rate of iliac artery stent placement was comparable to that of surgical bypass grafting.
Many series have studies various demographic and clinical factors for determining their relationship with primary stent patency. However, it is hard to conclude that any of those factors have a constant and proven positive relation with stent patency. The results of the aforementioned studies are affected by individual study design and the statistical analysis. In our study, the lesions at the EIA or the lesions that involved both the CIA and the EIA showed poorer primary patency than did the lesions in the CIA only. This is because the EIA is smaller in diameter and it is more likely to have diffuse disease when compared with the CIA. Although several multivariate studies have failed to show the effect of the anatomic location of a lesion on stent patency (32), lesions at the external iliac artery are generally known as a poor predictive factor for primary stent patency (33, 34). Johnston has reported that the predicted 3-year success rate was 73% for the patients with good run off and 30% for those patients with poor runoff in 58 PTAs of both the common iliac artery and the external iliac artery (33). In our series, the total run off score showed a positive correlation with primary stent patency on the Cox regression model. Because most of the patients with a poor runoff vessel underwent simultaneous or subsequent (less than one year) bypass surgery (35%) in our series, this might have contributed to the relatively better 5-year patency rate than was seen in other reports. Stent diameter also showed a positive correlation with primary stent patency on the Cox regression model. In this study, it is unique that the stents having the same or larger diameter than 10 mm showed a 9.1% higher occlusion hazard rate than did the stents having a diameter below 10 mm. It is possible that a stent more than 10 mm in diameter is a burden for the Asian population when considering their relatively smaller vessel size.
Our data indicate that none of the clinical risk factors, including age, diabetes, hypertension and smoking, showed a statistically significant influence on stent patency. We defined a smoking history as a current smoker or as a person who had abstained from smoking for 10 years or less prior to their stenting procedure. All the patients denied smoking after stenting, so we could not estimate the result of the relationship between current smoking and stenting. However, some of the patients with a smoking history probably continued to smoke.
In a study by Murphy and others that concentrated on disease distribution, they concluded that the patency rates for stenosis and occlusions were similar (35, 36); moreover, diffuse disease produced the worst results, and this conclusion was also reached by Dyet et al. (37). Long and his colleague's also reported good primary and secondary patency rates for occlusions (38), as did Blum (39). Although these variables were previously found to be significant in an angioplasty series (6, 33, 40) and also in a stenting series (41), our study showed that the lesion shape and distribution such as diffuse disease, obstruction, and the SCVIR classification did not affect the long-term outcome of stenting.
In a series involving iliac angioplasty alone, Johnston et al. have found a lower patency rate for women on a subanalysis of the external iliac stenosis (6, 33). The women's smaller vessel size has been suggested to be a possible reason for the decreased patency rates in women. However, gender was not analyzed in our study because the study population contained only 0.03% female patients. The number of stents used in one limb and also the stent type were not found to affect patency in our present study.
Intra-arterial pressure measurements can provide definitive information on the significance of a lesion. A commonly accepted threshold of abnormality is a drop in the systolic pressure of > 10 mm Hg (42). Indications for selective stenting following angioplasty include a residual systolic pressure gradient across the lesion of > 10 mm Hg at rest or > 20 mm Hg after vasodilator challenge (43). We obtained the same cutoff value, but the pressure gradients of all the cases were not obtained; therefore, we could not apply pressure gradient measurements to the multivariate Cox model. However, the changes of the transstenotic pressure gradient were statistically significant on paired t testing (p = 0.00).
Doppler US is used to follow iliac arterial stenting at most institutions. Uberoi et al. have used Duplex US during follow-up after stenting. They used the criteria of a significant stenosis as either a visible lumen reduction of > 50% on power Doppler US or as more than a doubling of the peak systolic velocities (> 2.5) (44). The angular course of the iliac artery limits the use of the peak systolic velocity. Moreover, any direct visualization of the vessel patency on power Doppler US was limited due to pelvic bowel gas, and the results could also be variable according to the US machine. We also found that the monophasic waveform of the CFA in the immediate phase was predictive of stent stenosis.
The limitations of our study were an insufficient number of patients in the subgroup analysis such as for the pressure gradient data, the ABI follow up data and the Doppler ultrasonography data. Not all the patients had full data in these categories and the application of the statistical analysis was limited. Further, this study was conducted in a retrospective fashion. From a statistical view point, including too many independent variables in the multivariate analysis can led to diminishing the testing power of the Cox regression analysis. In addition, not all the patients had objective imaging follow up results and some of the follow up data was based on clinical/noninvasive examinations for determining the patency of the stents. Determination of patency without using a definitive imaging modality always has pitfalls because the symptomatic aggravation does not always reflect stent obstruction itself. Peripheral disease progression can also be present without compromising the stent patency. Yet on the other hand, symptomatic well being does not necessarily represent good stent patency. The relative decrease in daily activity that is due to the aging process or to other physical condition can make the patient less sensitive to any symptomatic aggravation. The degree of collateral vessel development is another variable for symptom aggravation with or without it compromising the stent patency.
In conclusion, our study indicates that a relatively high level of long-term primary patency can be achieved for at least five years by performing iliac arterial stenting. However, the presumable 10-year patency was found to be worse than that of bypass surgery. Additionally, lesions involving the EIA or both the EIA and the CIA were poor prognostic factors for the primary stent patency. A poor run off score also diminished the primary stent patency. A stent larger than 10 mm in diameter is probably not recommendable for the Asian population because their actual arterial diameter is somewhat small. As isolated variables, none of the demographic and clinical factor had an influence on the outcome of stent patency. Further long term study with a full backdrop of imaging data will be needed to determine the variable data on long term patency rates.
Go to :
 XML Download
XML Download