

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Moyamoya disease involves slowly progressive stenosis in bilateral proximal intracranial vessels, leading to reduced cerebral perfusion (1, 2). Symptoms such as headaches and unilateral or bilateral transient ischemic attacks develop in young children, especially during hyperventilation (2, 3). Although the exact cause of the disease is still unknown and the specifics of its natural course are a matter of controversy, its outcomes range from reversible ischemia to cerebral infarction associated with permanent neurological deficits and intellectual impairment (4, 5). Early diagnosis followed by accurate treatment is, therefore, critically important, especially for young children.
Revascularization surgery in pediatric patients with moyamoya disease has been shown to be an effective treatment method (6, 7). At present, cerebral or MR angiography and MR imaging are modalities by means of which the disease can be diagnosed with confidence; in addition, single photon emission tomography (SPECT) provides confirmation of the diagnosis and is used to evaluate the cerebral perfusion reserve.
Localized proton MR spectroscopy (1H-MRS) has recently been used to detect the metabolic changes occurring in the brain in numerous diseases (8). Its noninvasive nature has increasingly attracted the attention of pediatricians, who see it as a promising application (9, 10). Although localized 1H-MRS has been used in patients with internal carotid artery flow lesions (11), it has never been employed in those with moyamoya disease. In regions without infarction but with severely reduced internal carotid flow, 1H-MRS has demonstrated decreased NAA/Choline ratios and a high incidence of cerebral lactate (11), and it can be inferred that in the brains of patients with moyamoya disease, NAA and/or Choline levels are lower than normal. In this study we used localized 1H-MRS to measure changes in the cerebral metabolite levels found in moyamoya disease before and after revascularization surgery. Our hypothesis is that localized 1H MRS can be used to preoperatively evaluate cerebral metabolic abnormalities, and to monitor these postoperatively.
MATERIALS AND METHODS
Subjects
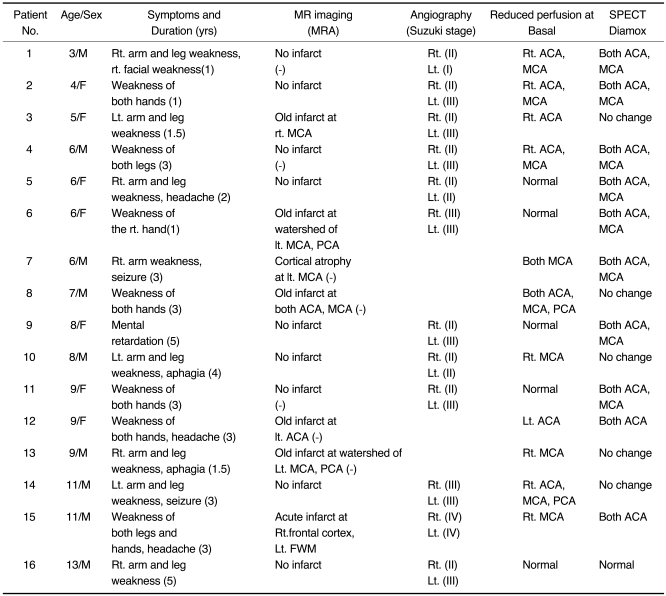
Our study group consisted of 16 consecutive children aged 3-13 (mean, 7.6) years in whom moyamoya disease was diagnosed between March 1998 and December 1999, and eight age-matched normal controls aged 4-11 (mean, 8) years. Diagnosis was based on the findings of conventional angiography (n=12), MR imaging (n=16), MR angiography (n=7), SPECT (n=16), and clinical symptoms. Nine children showed unilateral symptoms of transient ischemic attack and six had bilateral symptoms; at the time of initial diagnosis, these included TIA (n=15), headache (n=3), seizure (n=2) and/or aphasia (n=2). All patients underwent initial 1H-MRS, and four underwent follow-up 1H-MRS 6-19 months after surgery (encephalo-duro-arterio-myo-synangiosis; EDAMS). In three patients (numbers 1, 4, 11), revascularization surgery was performed in both hemispheres, and in one (number 7), in the left hemisphere only. These four patients underwent follow-up SPECT 6-22 months after surgery.
All patients and normal controls gave their informed consent to 1H-MRS. The study protocol conformed to the ethical guidelines of the 1975 Declaration of Helsinki, as reflected in its approval by our institution's Human Research Committee.
MRI, MR Angiography, Cerebral Angiography, and 99mTc-ECD SPECT
For MR imaging and angiography, a 1.5T scanner (Magnetom Vision, Siemens, Erlangen, Germany) was used, and in all patients, T1-weighted (TR/TE:600/11-20) and T2-weighted (TR/TE:3500/102) spin-echo images, as well as Gd-DTPA (Magnevist, Schering, Germany)-enhanced T1-weighted images, were acquired. In seven patients, MR angiography with a three-dimensional time-of-flight (3D-TOF) sequence was performed.
Twelve patients underwent transfemoral cerebral angiography using an Integris BN 3000 biplane (Philips Medical System, Eindhoven, Netherlands), after injection of the bilateral internal and external carotid and unilateral vertebral artery. Grading of the involved vessels was based on Suzuki's classification (3).
Using a Triad XLT20 (Trionix, Twinsburg, U.S.A.) equipped with a LEUR collimator interfaced to a Sun Sparc workstation, serial dynamic SPECT scans (1min×50 frames) were obtained in 16 patients. Two doses of 99mTc-ECD (ethyl cysteinate dimmer) were administered, one at the onset of scanning (20mCi) and one at 30 mins (20mCi). Diamox (1g) was injected intravenously at 10 mins. Two nuclear physicians visually assessed the perfusion status, comparing it with that of cerebellar perfusion.
Localized 1H-MRS
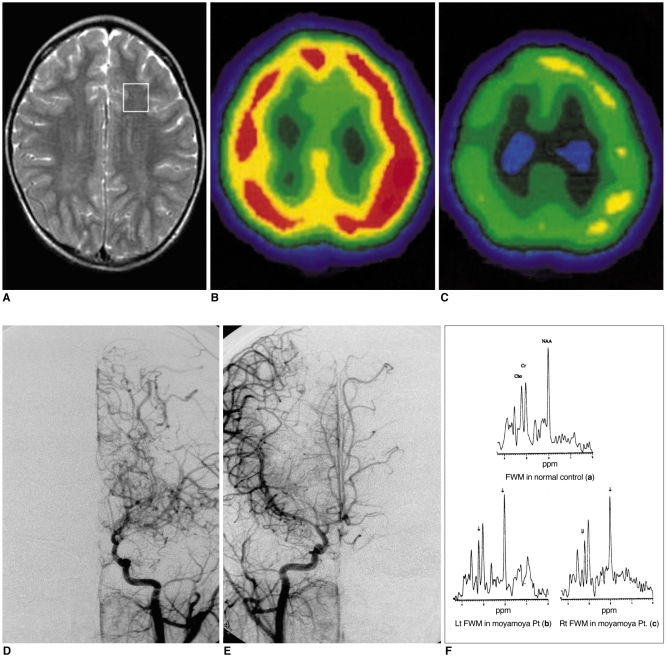
Using a 1.5T system (Signa; GE Medical Systems, Milwaukee, U.S.A.) equipped with shielded gradients, localized in-vivo 1H-MRS was performed 1-2 weeks after T2-weighted MRI was used to localize and evaluate any changes in brain parenchymal signal intensity, compared to previous MRI findings. Image-guided STEAM spectra were obtained from frontal white matter at the border zone between anterior and middle cerebral artery territory and the basal ganglia in both hemispheres, avoiding areas of old infarcts or abnormal signal intensities (Figs. 1A, 2A). The spectroscopic acquisition parameters were as follows: TR=3.0 sec/ TE=30 msec, and NS=36 AVG with PROton Brain Exam (PROBE) (GE Medical Systems). Voxel volumes were 7-9 ml, and a 3-pulse CHESS (CHEmical Shift Selective) sequence was used for suppression of the H2O signal.
All raw data were transferred to a Sun Sparc-10 work-station (SUN Computer Inc., Sunnyvale, U.S.A.), and processed using Spectral Analysis/General Electric (SA/GE) software (GE Medical Systems) incorporating low frequency filtering of residual water signal, apodization by 0.5 Hz of exponential line broadening, zerofilling of 8k, Fourier transformation, and lorenzian to gaussian transformation according to the scheme described by Kreis et al. (12). Metabolic peaks were fitted by the lorenzian line shape at known frequencies of N-acetylaspartate (NAA) at 2.02 ppm, creatine (Cr) at 3.03 ppm, choline and choline-containing compounds (Cho) at 3.22 ppm, and myo-Inositol (mI) at 3.56 ppm. The values of the [NAA/Cr], [Cho/Cr], and [mI/Cr] ratios were calculated.
Assessment
The spectroscopic data were expressed as mean±standard error. Mean (right and left) metabolite ratios between patients and normal controls, and between symptom-related and other hemispheres were compared using the Mann-Whitney U test. In four patients, changes in metabolite ratios after surgery were assessed by Wilcoxon's signed rank test. For statistical analyses, SPSS Windows (SPSS for Windows, SPSS Inc., Chicago, U.S.A.) was used.
RESULTS
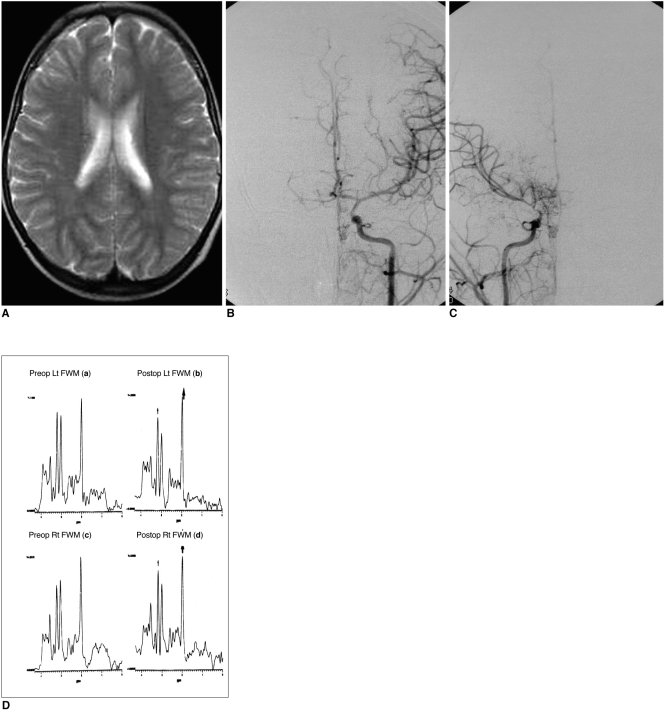
Tables 1 and 2 summarize the clinical data and findings at MR imaging, angiography, SPECT, and 1H-MRS (Figs. 1, 2).
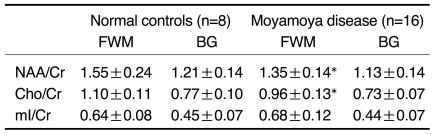
Localized 1H-MRS revealed decreased NAA/Cr and Cho/Cr ratios(Fig. 1F) in 16 patients, in whom mean NAA/Cr, Cho/Cr, and mI/Cr ratios were 1.35±0.14, 0.96±0.13, and 0.68±0.12, respectively, in frontal white matter, compared with 1.55±0.24, 1.10±0.11, and 0.64±0.08 in normal controls (p<0.05). In patients, mean NAA/Cr, Cho/Cr, and mI/Cr ratios were 1.13±0.14, 0.73±0.07, and 0.44±0.07, respectively, in both basal ganglia, while the corresponding figures for normal controls were 1.21±0.14, 0.77±0.10, and 0.45±0.07. Reduced NAA/Cr and Cho/Cr ratios were detected in 13 patients, while in three, the Cho/Cr ratio had increased. In two of these three, the NAA/Cr ratio had decreased, and in one it was normal.
In the symptomatic hemisphere, NAA/Cr, Cho/Cr and mI/Cr ratios were 1.35±0.28, 0.89±0.26, and 0.67±0.18, respectively, while on the asymptomatic side, the respective readings were 1.33±0.28, 0.93±0.24, and 0.68±0.22. The differences between the two hemispheres were not statistically significant.
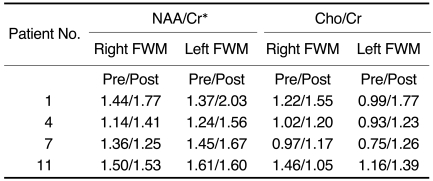
Four patients underwent follow-up 1H-MRS 6 to 19 months after revascularization surgery: their NAA/Cr ratios had increased (p < 0.05), slightly overshooting Cho/Cr ratios in the hemispheres (Fig. 2D) with improved symptoms of transient ischemic attack (Table 3). One of the four patients (number 7, Table 3) still exhibited TIA symptoms on the side not operated on, and the NAA/Cr ratio in frontal white matter remained low. Cho/Cr ratios were slightly overshot in all four patients, but were still within the upper normal limit. Basal and diamox stress SPECT showed increased perfusion in both hemispheres of all four patients, as compared with the preoperative results.
DISCUSSION
N-acetylaspartate is known to be a neuronal marker, and a decrease in its level indicates a loss of neurons or neuronal activity owing to myelin breakdown, as occurs in brain infarct, tumor, and radiation injury (13). Choline appears to contain contributions from phosphorylcholine and glycerophosphorylcholine, which are, respectively, a precursor to cell membrane and a product of its breakdown. An increased choline signal is therefore thought to be an indicator of active demyelination (14).
Duijin et al. (15) and Lanfermann et al. (16) observed decreased choline levels in chronic, but not acute or subacute, infarctions. In their study, they also observed that choline and creatine decreased to a lesser extent than N-acetylaspartate in the peripheral region of the infarcted lesion. This may explain the loss of neuronal function while glial cellular structure in the peripheral region is still intact. In our patients, the abnormal NAA/Cr and Cho/Cr values found in frontal white matter may also indicate a loss of neuronal function, a hypothesis supported by the normal MRI findings and absence of a lactate peak. A lactate signal is an end product of anaerobic glucose metabolism, suggesting that this ischemic process may be more likely in the chronic than in the acute state.
Children with moyamoya disease suffer from headache and unilateral or bilateral transient ischemic attack (2, 3), even if they do not have persistent neurological deficits. Decreased cerebral blood flow and cerebral perfusion reserve have been demonstrated in patients with the disease, and these lead to ischemic neurologic symptoms (17-25). CT and MRI are useful for the detection of infarction, but their ability to detect perfusion disturbances is limited. SPECT demonstrates the degree and region of hemodynamic compromise and is commonly used to determine suitable surgical candidates. It cannot, however, disclose metabolic change as a consequence of chronic cerebral ischemia. As shown in this study, 1H-MRS, which is noninvasive, can provide information on deranged metabolites under conditions of chronic cerebral hypoperfusion.
In this study, the findings of 1H-MRS appear to suggest a slightly greater decrease in Cho/Cr ratios in symptom-related hemispheres, but the differences were not statistically significant. Further investigation involving a large series with asymmetric involvement of both hemispheres would help clarity this issue.
In three of 16 patients, Cho/Cr ratios had increased and NAA/Cr ratios had decreased or were normal. Rutgers et al. (26) described the cerebral metabolic changes observed at 1H-MRS in patients with symptomatic occlusion of the internal carotid artery. During the period of acute infarction, the NAA/Cr ratio was significantly lower than in control subjects in the hemisphere ipsilateral to ICA occlusion, and the Cho/Cr ratio was significantly higher. Subsequently, the Cho/Cr ratio decreased significantly and returned to the control value. These findings suggest that increased Cho/Cr ratios may indicate an acute process.
Various revascularization procedures such as EDAMS have served to increase the blood supply to ischemic areas of the brain, and in this study, symptoms of transient ischemic attack disappeared or improved in three patients after revascularization surgery, and NAA/Cr ratios increased. Increased N-acetylaspartate levels have been recognized only in Canavan's disease and in infants during normal development (27, 28), and could account for changes in N-acetylaspartate metabolism and/or neuronal activity (29). In this study, another finding after revascularization surgery was that Cho/Cr ratios had slightly overshot. It has been reported that the choline levels increased to above the normal limit after liver transplantation and that this was due to cyclosporine related encephalopathy or neurotoxicity (8). The patients in our study did not, however, undergo immunosuppressive treatment, and it can therefore be inferred that increased perfusion after revascularization surgery may transiently influence the level of choline. Further study and long-term follow-up of choline levels are therefore needed.
It has been shown that in moyamoya disease, vascular reserve in the cerebral cortex of anterior and middle cerebral artery territory is significantly lower than in posterior cerebral artery territory and the central region around the basal ganglia and thalami (30-32). The results of our study indicated that in both basal ganglia, metabolite levels were normal, though it may be speculated that metabolic change might occur there at a later stage of the disease, when basal collaterals disappear.
In conclusion, localized 1H-MRS in patients with moyamoya disease demonstrated bilaterally decreased N-acetylaspartate and choline ratios. 1H-MRS effectively measures the metabolic changes occurring in the brain in moyamoya disease, and its non-invasive nature lends itself to the preoperative evaluation of metabolic abnormality and its postoperative monitoring.
 XML Download
XML Download