

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Thymic epithelial tumors (thymoma and thymic carcinoma), derived from the thymic epithelium, show variable histologic features and heterogeneous oncologic behavior. Various systems of histologic classification of these tumors have been implemented, leading to confusion regarding the nomenclature employed (1). In an effort to establish a universal classification system which reflects the invasiveness and prognosis of thymic epithelial tumors, the World Health Organization (WHO) proposed, in 1999, a consensus classification (2).
Although there is some degree of overlap among the various types of tumor included in the new WHO classification, the CT and MR findings of thymic epithelial tumors help differentiate their various subtypes (3-5). The purpose of this pictorial review is to describe, on the basis of the new WHO classification, the CT, MR and pathologic findings of the various subtypes of thymic epithelial tumors.
HISTOLOGICAL FEATURES AND PROGNOSIS
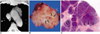
The histologic features of thymic epithelial tumors vary, their neoplastic epithelial cells showing differing shapes and degrees of atypia. In addition, various degrees of non-neoplastic lymphoid cells coexist with neoplastic epithelial cells within the tumors (2,6). Numerous classification systems for thymic epithelial tumors have been proposed but have fallen out of favor because the suggested morphologic types lacked consistent prognostic significance. In the mid 1980s, Muller-Hermelink et al. (7) proposed a new functional classification of thymomas based on their histologic and immuno-phenotypic resemblance to cortical or medullary areas of the thymus. The recently published WHO classification of thymomas adopted the Muller-Hermelink classification, but used alpha-numeric terms (3). The new system is based on the morphology of epithelial cells as well as the lymphocyte-to-epithelial cell ratio (Fig. 1): in thymomas are divided into two groups (type A and B) depending on whether the neoplastic epithelial cells and their nuclei are spindle-or oval-shaped (type A), or have a dendritic or epithelioid appearance (type B) (Fig. 2); type AB tumors are those which combine these two morphologies (Fig. 3). Type B tumors are further divided into three subtypes according to the proportional increase in their epithelial component and the emergence of atypical neoplastic cells (Figs. 4-6). All types of thymic carcinomas are classified as type C (Figs. 7, 8). The relationship between the new WHO classification and previous histologic classification systems is summarized in Table 1. The WHO classification reflects the clinical features of these tumors and correlates with prognosis. According to Okumura et al. (8, 9), type-B2 and B3 tumors show aggressive behavior compared with types A, AB, and B1 in terms of invasiveness, postoperative survival, and tumor recurrence. For type-A, AB, or B1 thymomas, there is more likelihood of complete resection than for types B2 or B3.
CT Findings
According to Tomiyama et al. (4), smooth contours and a round shape most strongly suggest a type-A tumor (Table 2) (Fig. 2); type-C tumors are significantly larger than types A and B2 (Figs. 2, 5, 7, 8); irregular contours and mediastinal lymphadenopathy are most suggestive of type C (Figs. 7, 8). Calcification is more frequently seen in type-B1, B2, and B3 tumors than in type AB and type C (Fig. 6). A high degree of homogeneous enhancement tends to indicate type A or AB (Fig. 2); heterogeneous enhancement is seen more often in types B3 and C (Fig. 8). Mediastinal lymphadenopathy is present in 43% of type C tumors, 7% of type AB, but not in other types of thymic epithelial tumors. This feature has, however, been found to be of limited value in differentiating types AB, B1, B2, and B3.
According to Jung et al. (5), CT indicated that atypical (type-B3) thymomas are significantly smaller (mean, 4.7 cm) than thymic carcinomas (type-C thymomas) (mean, 7.2 cm). Invasion of the great vessels, mediastinal lymphadenopathy, extrathymic metastases and phrenic nerve palsy occur only in patients with type-C thymic carcinoma (Figs. 7, 8). The frequencies with which necrosis, intratumoral calcification, pleural effusion, pleural implants, pericardial effusion, and obliteration of the mediastinal fat plane arise are not significantly different between the two types. Do et al. (10) reported that mediastinal lymphadenopathy was present in 40% of thymic carcinomas (type-C thymoma) and 8% of invasive thymomas. With regard to the latter, they did not, however, classify the histopathologic types. Pleural seeding is seen in type-B and C tumors (Figs. 5, 8), but not in type A or AB (5, 10).
MR Findings
At T1-weighted MR imaging, types-A, AB, and B1 thymomas show signal intensity similar to (11) or slightly higher than that of muscle (12-15), while T2-weighted imaging demonstrates signal intensity higher than that of muscle but similar to that of fatty tissue. At Gd-DTPA-enhanced MR imaging, homogeneous and moderate enhancement is observed (Fig. 3). T1-and T2-weighted imaging both demonstrate that the signal intensity of type-B2 and B3 thymomas is the same as that of types A, AB, and B1 (14-17). At T2-weighted imaging, however, most B2 and B3 thymomas manifest inhomogeneous signal intensities with scattered high-intensity areas, shown at pathologic examination to correspond to cystic spaces with or without hemorrhage (14) (Figs. 5, 6). In a study by Sakai et al. (14), T2-weighted imaging indicated that six of 12 invasive thymomas (probably type B2 or B3 according to the WHO classification) had lobular internal architecture, with 1- to 2-mm-thick low-intensity lines (Fig. 6); for the five benign thymomas (probably WHO-type A, AB or B1), this was not, however, the case (Fig. 3). Pathologic examination showed that the lobular internal architecture consisted of round or irregular areas containing tumor cells separated by relatively thick fibrous septa (Fig. 6). Unlike type-A, AB, B1, B2, and B3 tumors, thymic carcinomas (Type C) show relatively low signal intensity at both T1- and T2-weighted MR imaging (15), appearing as slightly inhomogeneous lesions.
SUMMARY
The histologic appearance of thymic epithelial tumors, as described in the new WHO classification system, reflects the oncologic behavior of thymomas and thymic carcinomas. An awareness of the various CT and MR findings of the different types of thymic epithelial tumors, as reflected in the WHO histologic classification, may be helpful in clinical practice for the assessment and treatment of patients with thymoma and thymic carcinomas.









 XML Download
XML Download