

 PDF
PDF ePub
ePub Citation
Citation Print
Print


In patients with malignancy, obstruction of the superior vena cava and its tributaries is commonly encountered (1, 2); benign causes such as central venous catheters, high-flow states associated with hemodialysis access fistulas, intravenous pacemaker wires, and mediastinal fibrosis are less common. Benign thoracic central venous obstruction (i.e. obstruction of the superior vena cava, and brachiocephalic and subclavian veins) has, however, increased in frequency with the increasing use of central venous catheters and pacemaker leads.
Interventional radiologic measures are the primary treatments of choice in benign central venous obstruction, while the primary treatment for superior vena cava syndrome in patients with malignant disease is radiation therapy (1). The presence or absence of venous obstruction, and its cause, location, degree, and extent is thus important for the planning of treatment. With the advent of helical CT, CT venography can be a valuable modality in patients with superior vena cava obstruction (3).
We believe that if it can provide reliable information for excluding malignant causes, showing the extent and degree of venous obstruction and demonstrating venous thrombus, CT venography can facilitate interventional procedures. To our knowledge, however, no published study has assessed its usefulness in patients with benign thoracic central venous obstruction. The purpose of this study was to evaluate the role of CT venography under such circumstances, comparing its performance with that of digital subtraction venography.
MATERIALS AND METHODS
Patients
Between January 1994 and February 2002, 43 consecutive patients with suspected central thoracic venous obstruction underwent CT venography. Twenty-five were excluded because a malignant cause of this obstruction was established (n=15) or because digital subtraction venography had not been performed (n=10), and the remaining 18 were enrolled in this study.
Nine were male and nine were female, and they were aged between 11 and 71 (mean, 49) years. All except one complained of edema of the face and/or upper extremities. Ten had a functioning hemodialytic fistula at the upper ipsilateral extremity, and five others had a history of central venous catheterization for hemodialysis (n=3), chemotherapy (n=1), or pacemaker insertion (n=1). In one other, Behcet's disease had been diagnosed. For the review of patients' records or images, our institutional review board requires neither that its approval be given, nor the informed consent of the patients involved.
CT Venography
For CT examinations, a Somatom Plus S and a Somatom Plus 4 (Siemens, Erlangen, Germany), and an MX8000 multidetector row CT scanner (Marconi Medical Systems, Cleveland, Ohio, U.S.A.) were used. First, unenhanced images were obtained from lower neck level to diaphragm level, with parameters of 10 mm beam collimation, 10 mm/sec table speed, 5 mm slice thickness, and a 5 mm reconstruction interval. The findings were used to determine the scanning range of CT venography. For the Somatom Plus S and Plus 4 scanners, the CT parameters for CT venography were 3 mm beam collimation, 5-6 mm/sec table speed, 3 mm slice thickness, and a 2 mm reconstruction interval. From the level of the first thoracic vertebra to that of the upper one-third of the right atrium, the scanning range was 16-18 cm and scan time was 30-32 seconds. For the MX8000 scanner, the parameters were 2.5 mm detector collimation, 20 mm/sec table speed, 3.2 mm slice thickness, and a 1.6 mm reconstruction interval. From the level of the mandible angle to the level of the upper abdomen, the scanning range was 28-34 cm and scan time was 14-17 seconds. In all patients, CT venography was accomplished during a single breath-hold.
Diluted contrast medium (200 mL) was prepared by mixing nonionic iopromide (Ultravist 370; Schering, Berlin, Germany) and sterile isotonic 0.9% saline solution in a ratio of 1:2. Using a mechanical injector, this was injected simultaneously into either both upper extremities (n=6) or only into a diseased upper extremity (n=12). When the suspected level of venous obstruction was a unilateral subclavian or brachiocephalic vein, the medium was injected ipsilaterally (unilaterally) into a diseased extremity at a rate of 3 mL/sec. When the suspected level of venous obstruction was the superior vena cava, or a bilateral subclavian or brachiocephalic veins, the medium was injected bilaterally into each extremity at a rate of 2 mL/sec. A total of 200 mL was injected bilaterally, and 180 mL unilaterally. Thus, for each extremity, the duration of injection was 50 seconds for bilateral injection and 60 seconds for unilateral injection. To achieve sufficient enhancement of collateral vessels and central thoracic veins, scanning was delayed for as long as possible, which was 20-40 seconds.
Delayed-phase CT scanning involved 5 mm slice thickness and 60-80 seconds' delay. The data were transferred to a personal computer, and using a three-dimensional software program (Rapidia®, INFINITT, Seoul, Korea), maximum-intensity-projection, multiplanar-reformation, and volume-rendering reconstructions were obtained.
Digital Subtraction Venography
In all patients, digital subtraction venography was performed within two days of CT venography. To facilitate interventional procedures, direct-catheter venograms were obtained in 14 cases. The access route was determined according to the site, degree, and extent of obstruction, as per the findings of CT venography. For example, in subclavian vein stenosis or obstruction, access was via the brachial vein, and in brachiocephalic vein stenosis, via the femoral vein. For the treatment of complete occlusion of the superior vena cava or left brachiocephalic vein, access was via the internal jugular vein. In four patients, no interventional procedure was performed; an intravenous route was established via the dorsum of the hand, and ascending venograms thus obtained.
Image Analysis
To evaluate the degree of central venous obstruction, two radiologists (H.C.K., J.W.C.) retrospectively interpreted each CT venogram, and an experienced vascular radiologist (J.H.P.) reviewed the digital subtraction venograms. The order of examination was random, the patient's name was hidden, and each radiologist was blinded to the findings of other examinations. Digital subtraction venography was considered as the gold standard. In each case, the projection that demonstrated the most severe stenosis was used, and the sites of stenosis were addressed. The diameter at the site of the most severe stenosis was divided by the arbitrary normal value determined after consideration of the diameter of the proximal and distal vein beyond the stenosis; the resulting value was subtracted from one and then multiplied by 100 to yield the percentage of stenosis according to the diameter of the vessel. For each vein, stenosis was graded as follows: 0 (1-49%), insignificant stenosis; I (50-74%), moderate stenosis; II (75-99%), severe stenosis; III, complete occlusion; or IV, dynamic obstruction (i.e. stenosed at inspiration and occluded at expiration).
In addition, the extent of venous obstruction and the presence or absence of thrombus, as observed at CT venography, were analyzed by two independent reviewers (H.C.K, J.W.C.), and another reviewer (J.H.P) analysed these features by assessing the findings of digital subtraction venography. Segmental obstruction was defined as "short" if less than 2 cm, and "long" if 2 cm or more.
The causes of benign central venous obstruction, as seen at CT venography and digital subtraction venography, was determined by experienced vascular radiologists (J.W.C., J.H.P), and the exact causes of venous obstruction were determined by these two readers according to the information obtained during imaging studies and interventional procedures, and surgicopathologically. In all cases, decisions were consensual.
The implications of the findings of helical CT venography for treatment planning and interventional procedures were assessed by J.W.C., who, on the basis of these findings, determined the venous access site and performed the interventional procedures.
Statistical Assessment
To compare CT venography and digital subtraction venography in terms of categories of stenosis, analysis using the Spearman rank correlation coefficient (Rs) was performed. For CT venography, the extent of agreement between observers in their interpretation of the degree of obstruction was determined using the κ coefficient. Agreement was classified as mild (κ > 0.40-0.69), good (κ > 0.70-0.89), or excellent (κ > 0.90-1.00). Statistical analyses were performed using computer software (SPSS, version 10.0; SPSS, Chicago, Ill., U.S.A.), and a p value of less than 0.05 was considered statistically significant.
RESULTS
Degree of Obstruction
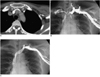
At CT venography, both readers identified all the 24 stenotic sites demonstrated at digital subtraction venography. Fourteen patients had one stenotic site, three patients had two, and one patient had four; the degree of obstruction was grade I at three sites, grade II at ten, grade III at nine, and grade IV at two. Interobserver agreement was good (κ=0.864). Regarding the degree of stenosis, there was significant correlation between CT venography and digital subtraction venography (reader 1: Rs =0.58, p < 0.01; reader 2: Rs = 0.56, p < 0.01). Reader 1 underestimated two cases of complete occlusion as severe stenosis (Fig. 1), and reader 2 underestimated one such case as severe stenosis and overestimated one case of severe stenosis as complete occlusion. In two patients with dynamic obstruction due to extrinsic compression of the left brachiocephalic vein, both readers reported moderate or severe stenosis at CT venography (Fig. 2).
Extent of Venous Obstruction and Thrombosis
Segmental obstruction was short in 14 patients and long in four, and in four venous thrombosis was noted. CT venography accurately demonstrated the proximal and distal extent of venous obstruction and the presence or absence of thrombi, and in these respects, interobserver agreement was complete. At digital subtraction venography, the proximal extent of stenosis in three patients with long segmental obstruction was not demonstrated, and in two of the four with venous thrombosis, this appeared as filling defects. In two patients with focal stenosis and associated thrombi, furthermore, the latter were not depicted.
Causes of Obstruction
The causes of obstruction were intrinsic narrowing (n=10) (Figs. 1, 3), extrinsic compression of the left brachiocephalic vein between the sternum and arch vessels (n=5) (Fig. 2), venous thrombosis (n=2), and mediastinal inflammatory pseudotumor (n=1). CT venography accurately diagnosed the causes of obstruction in all patients, but digital subtraction venography failed in this respect in five patients (two with extrinsic compression, one with an inflammatory pseudotumor, one with pacemaker-induced superior vena cava obstruction associated with thrombosis, and one with Behçet's disease and diffusely obliterated thoracic central veins). In the patient with an inflammatory pseudotumor confirmed at post-surgical histopathologic examination, CT venography demonstrated an enhancing mass with internal calcification encasing the superior vena cava.
Implications for Treatment
Among the 14 patients who underwent interventional procedures, venous access was via the brachial vein (n=7), femoral vein (n=4), internal jugular vein (n=2), or both the internal jugular and brachial vein (n=1). In no case did the access route give rise to problems during the procedure. Without the information provided by CT venography, we would have routinely punctured the brachial vein of all patients; thus, access to this information meant that a different access route was chosen in half of all cases.
In one patient, CT venography clearly demonstrated focal stenosis of the left subclavian vein, which was obscured by an overlapping collateral vein, and for this same reason, ascending venography underestimated the extent of the stenosis (Fig. 3). Its presence was confirmed, however, at direct-catheter venography performed on the basis of the CT venographic findings.
In two patients with membranous obstruction, we were able to blindly puncture the membrane and perform balloon angioplasty: CT venography had clearly depicted the orientation of the membrane and the anatomical relationship between the proximal and distal venous segments (Fig. 1).
DISCUSSION
The presence of a central venous catheter and high blood flow from arteriovenous fistulas are major causes of benign thoracic central venous occlusion (4). Central venous stenoses or occlusions in patients undergoing hemodialysis are thought to originate from high-flow states, and occur at sites of turbulence such as valves (4), and injury due to the insertion of a temporary dialysis catheter has also been recognized as a risk factor for central venous obstruction (6). In our series, most cases involved arteriovenous fistulas, indwelling catheters, or pacemaker leads.
In this study, we identified another important cause of benign thoracic central venous obstruction, namely extrinsic compression of the left brachiocephalic vein between the arch vessels and the sternum. Long-standing hypertension and volume overload in chronic renal failure may elongate and dilate the aorta and arch vessels, and this can reduce the presternal space and cause extrinsic compression of the left brachiocephalic vein. A case in which this occurred was reported a decade ago (7), but the routine use of CT venography would probably show that the condition is more frequent than might be assumed. At digital subtraction venography in cases in which obstruction was not complete, extrinsic compression appeared as an obliquely running band compressing the left brachiocephalic vein. However, complete obstruction made it difficult to recognize extrinsic compression. Digital subtraction venography also demonstrated that when the obstruction caused by extrinsic compression was incomplete, its degree changed dynamically according to the respiration cycle; CT venography, however, failed to demonstrate this dynamic change. Since inspiration elevates the sternum, and widens the antero-posterior dimension of the thorax and relieves extrinsic compression, CT venography or digital subtraction venography performed during inspiration may underestimate the degree of stenosis accompanying extrinsic compression of the left brachiocephalic vein.
One of the advantages of CT venography over digital subtraction venography is its ability to evaluate the proximal extent of obstruction or thrombosis. In our series, CT venography with a long delay time clearly depicted the status of the proximal central vein, even where there was complete occlusion. In three patients with long segmental obstruction, however, digital subtraction venography performed with the catheter distal to the obstruction failed to accurately demonstrate the vein's proximal extent. This could be determined by passing a catheter beyond the obstruction, but if this is unsuccessful, venous access at a different site is required. The superiority of CT venography over digital subtraction venography seems to be related to the longer duration of contrast injection required by the former, as well as its longer scan delay time and greater contrast resolution. A further advantage of CT venography is its ability to provide three-dimensional images at any desired viewing angle. In our series, CT venography using axial projection or cranio-caudal angulation revealed hidden stenotic foci behind a large overlapping collateral vein.
Benign central venous obstruction is treated mainly by radiological intervention, which can involve percutaneous balloon angioplasty, intravascular stent placement, and transcatheter thrombolysis and mechanical thrombectomy (8-10). For treatment planning, interventional radiologists require as much information as possible, and in our study, CT venography revealed the severity, extent and cause of central venous obstruction, as well as the presence or absence of venous thrombosis. With this information, it was possible to select candidates for radiological intervention and determine the most suitable venous access route for the procedure. We were, in addition, able to prepare the necessary devices (such as a stent of suitable diameter and length), and medication, before initiating interventional procedures.
CT venography, however, suffers certain technical limitations. In patients with central venous obstruction and severe edema of the upper extremities, for example, venous puncture may be difficult. In addition, the spatial resolution of CT venography is lower than that of digital subtraction venography, and in cases involving severe stenosis or occlusion, the former may over- or underestimate the grade of stenosis. Further problems which may arise are beam-hardening artifacts due to the inflow of contrast material, flow artifact due to the inflow of unopacified blood, and poor enhancement of proximal central veins beyond the obstruction or the blind stump, with very slow flow between the obstruction site and the origin of collateral vessels. In order to overcome these problems, we used diluted contrast material and a scan delay time which was as long as possible. By these means, CT venographic images adequate for diagnosis and for the enhancement of proximal central veins beyond the obstruction or the blind stump, were obtained in all patients. To reduce flow artifacts in the superior vena cava, bilateral injection may be better than unilateral, and in this study, we used ipsilateral injection in 12 patients with edema of one upper extremity. Although some flow artifacts were present in contralateral central veins and the superior vena cava, the information derived from CT venography was sufficient for diagnosis and treatment, and on the basis of the observed pattern of opacification of collateral and central veins, an understanding of the venous hemodynamics involved was facilitated.
Our study, too, suffered certain limitations. First, because patients in whom a venous lesion was diagnosed at CT venography underwent digital subtraction venography, it was affected by selection bias: a patient with a negative CT venogram and a positive digital subtraction venogram could not be included. Second, of 28 potentially eligible patients with benign causes of central venous obstruction, only 18 underwent digital subtraction venography. The decision to attempt interventional therapy was based on the results of CT, and this can also cause selection bias.
In conclusion, helical CT venography provides essential information about the cause, severity, and extent of obstruction, and is thus a useful diagnostic modality for the diagnosis and treatment of benign thoracic central venous obstruction.


 XML Download
XML Download